
Submitted by jer5150 on Sun, 03/31/2013 - 13:08
Patient's clinical data: 66-year-old white man.
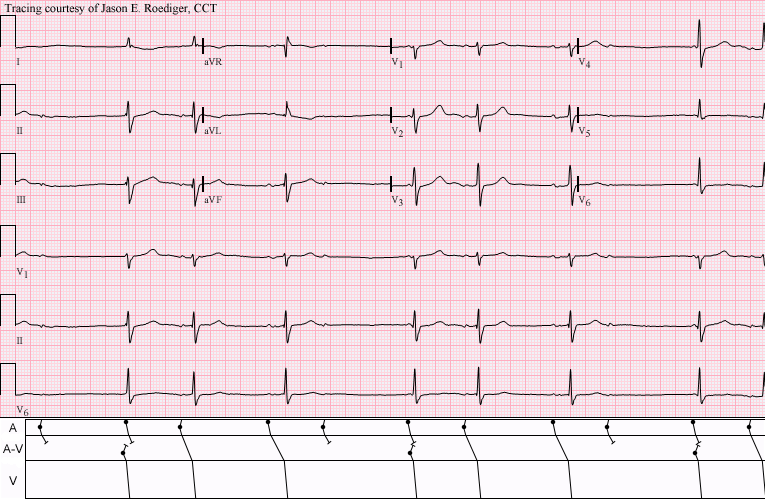
Amongst the computer's several statements was the interpretation of "Undetermined rhythm". To the computer's statement, the reviewing cardiologist added the freehand text of "Abnormally slow" but failed to provide a diagnosis.
What is accounting for this pattern?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Potential for Wenckebach?
The P waves dont seem regular to me, so I dont think that there is AV block.
Here is what I think:
Nonconducted P wave (propably PAC)
1st QRS complex = junctional escape beat with nonconducted sinus p wave hidden inside
2nd QRS = sinus
3rd QRS = sinus with longer PR
then = nonconducted PAC
4th = junctional escape with preceding nonconducted sinus P wave
5th = sinus
6th = sinus with longer PR
then = nonconducted PAC
7th = junctional escape with preceding nonconducted sinus P wave
So I would say, that there is potential for wenckebach, but the PAC´s prevent it from happening and also delay the next sinus P wave = and that´s why we see those junctional beats.
Dual SA/AV Wenckbach with AV Nodal Escape Beats
There is group beating that is not due to chance. Against PACs as the cause of the pauses is the relatively late occurence in the cycle of P waves. This is not simple AV Wenckebach because the atrial rate is not regular - but the group beating and seemingly increasing PR for some beats suggest (as per Jan) the "potential" for AV Wenckebach. All of which left me to ponder the possible additional role of SA block.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
INTERPRETATION
COMMENTS:Each sequence begins with a sinus beat conducted with a prolonged P-R interval. The sinus beat is followed by an APB that arrives at the A-V junction during its absolute refractory period (ARP) and is not conducted causing a “pause”. The pause is terminated by a junctional escape beat at a potential escape rate of 35/min that partially coincides with the next sinus impulse
Whether or not an APB is normally conducted or nonconducted depends almost entirely on the length of the preceding R-P’ interval.
Since the APBs bare a fixed “coupling” to the sinus impulse and NOT to the junctional escape, this has the effect of “pushing” the APB further to the right and thus lengthening the R-P’ interval to a duration where normal conduction is possible. This sets up a situation where the repetitive sequence repeats itself indefinitely until the pattern is disrupted by termination of the APBs.
The junctional escape is immediately preceded by a sinus impulse at an impossibly short P-R interval so it is therefore dissociated.
In lead II, the sinus P-waves have a "camel hump" appearance with the first hump being slightly bigger than the second hump. This second “hump” in the sinus P-wave can not be seen during the junctional escape beats because it occurs during the QRS complex. The P'-wave on the APBs has a diphasic appearance with the first component being negative and the second component being positive.
This patient had documented cases of nonconducted APBs and Type I A-V block (Wenckebach periodicity) on other serial ECGs.
Based on the duration of the sinus node recovery time (SNRT), the basic sinus rate is probably bradycardic.
An allorhythmia is defined as a repeated recurrence of an arrhythmic sequence. In this case we have a sinus beat (SB) conducted with prolonged P-R interval followed by a nonconducted APB, which is followed by a junctional escape (JE) beat dissociated from a sinus impulse, which in turn is followed by a normally conducted APB, and the sequence repeats itself – SB, Nonconducted APB, JE, APB, SB, Nonconducted APB, JE, APB, etc., etc.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]