
Submitted by Dawn on Thu, 10/16/2014 - 20:11
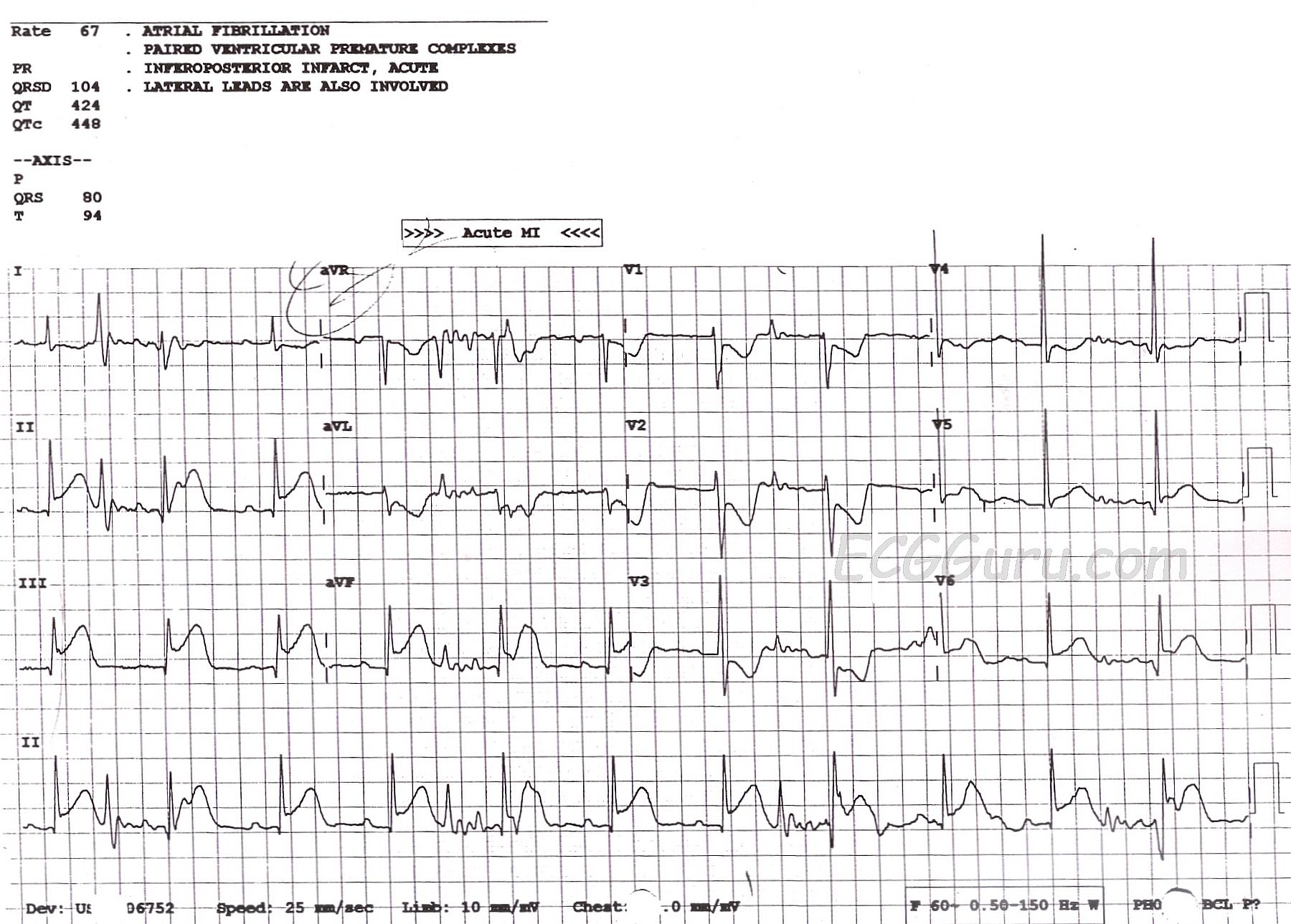
This ECG is taken from a 66-year-old man who presented to the Emergency Dept. with a complaint of chest pain. The ECG shows clear signs of acute inferior wall MI: ST segment elevation in Leads II, III, and aVF and reciprocal ST depression in Leads I and aVL. In addition, there are reciprocal ST depressions in Leads V1, V2, and V3. These indicate that the MI extends up the inferior wall into the area called by most clinicians the posterior wall. When the injured area extends high enough from the inferior wall, it becomes visible to the anterior-septal leads as ST depression. There is also a small ST elevation in Leads V5 and V6, the low lateral wall, indicating a common blood supply for the inferior and low lateral walls (usually the right coronary artery). All of these findings make this a rather "typical" inferior wall MI.
Unfortunately, this ECG also has a significant amount of artifact. The second, sixth, and tenth "beats" appear to be premature beats in Leads I and II. However, it is important to remember that the four channels on this ECG are run simultaneously. That is, any complex of significant voltage should show up four times. The "premature" beats do not appear in Lead III, and do not affect the timing of the appearance of the next beat at all. They also appear during moments of baseline disruption, indicating that they are not heartbeats, but simply artifact.
Why is this important? Artifact makes the ECG hard to interpret accurately. The ECG machine even had a difficult time, completely ignoring obvious P waves, and calling the rhythm "atrial fibrillation". Every effort should be made to obtain the cleanest, most artifact-free ECG possible.
Additional note: it can be very informative to do a right-sided ECG on an IWMI patient, or at least a V4Rt. In fact, it is a protocol requirement in many EMS agencies. Right ventricular infarction can change the hemodynamics of your patient, causing a need for fluid resuscitation. In fact, a drop in BP, such as that caused by nitroglycerin, can cause circulatory collapse. Ntg should be given cautiously to RVMI patients. Fortunately, IV fluids will seldom cause left heart overload in these patients. A look at the right ventricle with V4Rt can be very helpful in deciding treatment options.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.