
Submitted by Dawn on Sun, 03/04/2012 - 02:13
Our expert today is Dr. Ken Grauer. He is a frequent contributer to the ECG Guru.
KEN GRAUER, MD is Professor Emeritus (Dept. Community Health/Family Medicine, College of Medicine, University of Florida in Gainesville).
Dr. Grauer has been a leading family physician educator for over 30 years. During that time he has published (as principal author) more than 10 books and numerous study aids on the topics of ECG interpretation, cardiac arrhythmias, and ACLS (including an ongoing Educational ECG Blog.
Answer:
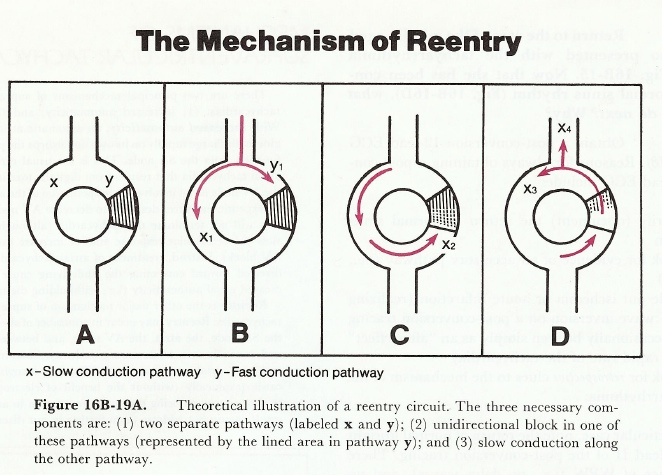
PSVT is a reentry tachycardia. This arrhythmia carries many names, one of which is AVNRT = AV Nodal Reentry Tachycardia - recognizing that in the vast majority of cases, there is reentry occurring in or around the AV node. The AV node is not a homogeneous structure - instead functionally (and anatomically on a microscopic level) - there are 2 basic pathways. One of these conducts "fast" - and the other "slower". Conduction preferentially goes down the "fast" pathway (thereby 'blocking' and preventing conduction down the slow pathway). But if for any reason (like a PAC) the fast pathway is "blocked" - then conduction of the impulse will have to go down the "slow" pathway. If the timing is just right - conditions may be set up that allow "reentry" within the AV node - with the impulse going down the slow pathway and up the fast pathway. Less commonly, reentry within the AV node may be set up in which the impulse goes down the fast pathway and back up the slow pathway.
Think of the phenomenon of reentry as comparable to the situation when 50 young children are all holding hands and running around in a circle while holding hands. All it takes is for one disgruntled person to stick out their leg - and ALL 50 of the children who are holding hands will fall down. So it is with reentry - it is a circuit that is set up by fortuitous circumstances of conduction speed, refractory period duration, and usually a precipitating premature impulse. How do we treat AV Nodal Reentry Tachycardia (PSVT)? Either by vagal maneuvers or medication such as adenosine, diltiazem/verapamil, or beta-blockers - ALL of which at least transiently alter conduction properties within a portion of the AV node. Just like the disgruntled citizen who stuck out their leg and tripped up all 50 children - all it takes is brief alteration/interruption of the conduction circuit (by meds or vagal maneuver) to terminate an AV Nodal Reentry Tachycardia.
Simplistic illustration of the concept of reentry appears in the Figure below (excerpted from pp 567-574 of Grauer K, Cavallaro D: ACLS: Comprehensive Review [Vol 2] - 3rd Edition, Mosby Lifeline, St. Louis - 1993). For a more detailed look at reentry - visit: https://www.kg-ekgpress.com/reentry-svt/ - where you can download a pdf of the above 7 pages.
Ken Grauer, MD ([email protected])
Exerpted from pp 567-574 of Grauer K, Cavallaro D: ACLS: Comprehensive Review (Vol. 2) - 3rd Edition, Mosby Lifeline, St. Louis - 1993.
Related Terms:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.