
Submitted by Dawn on Sat, 01/19/2013 - 16:22
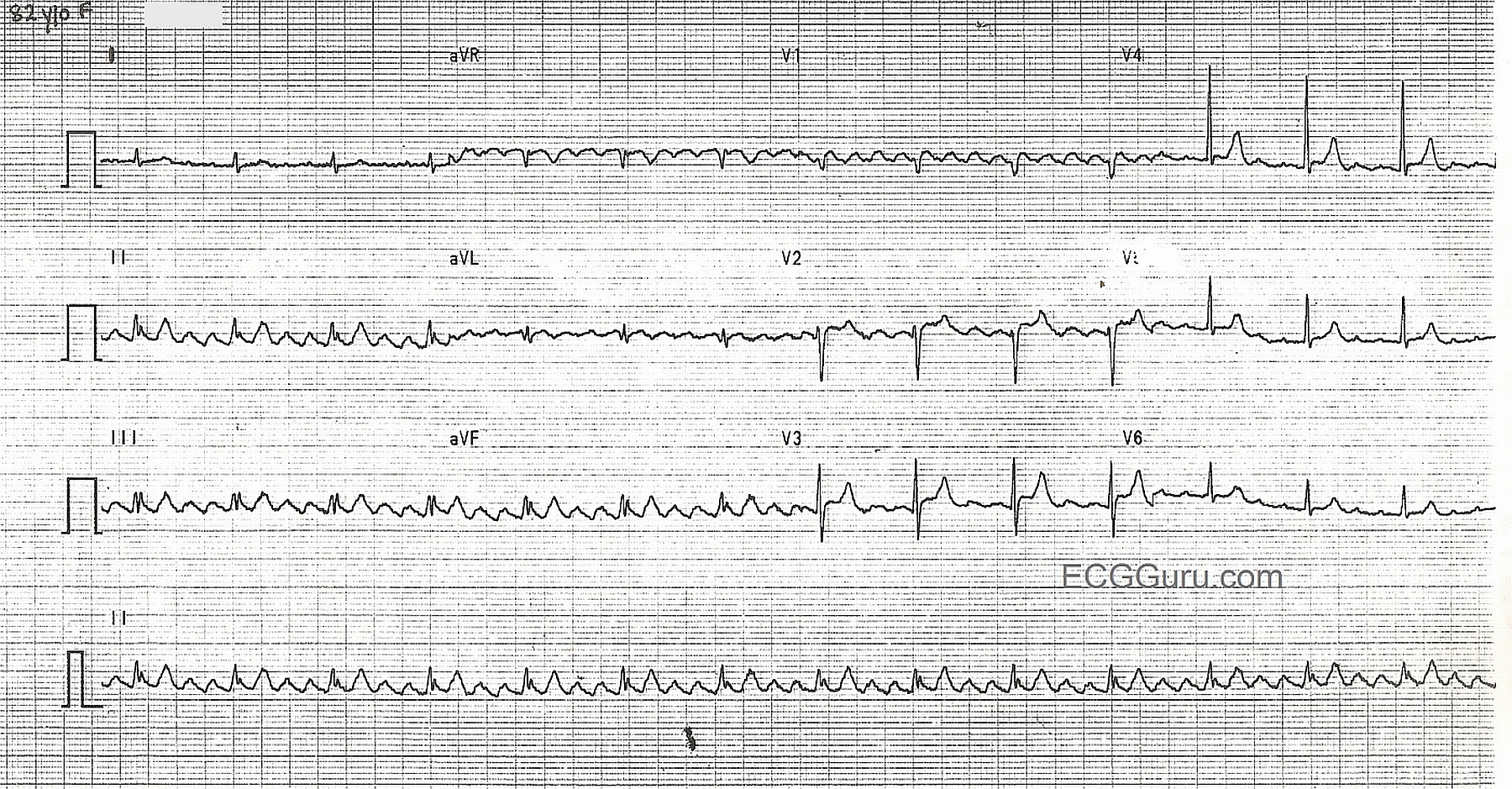
This nice example of atrial flutter offers many teaching opportunities. "Sawtooth" flutter waves are readily visible in Leads II, III, avF, and V1, typically good "P wave" leads. Other leads show small, discreet P waves that the beginning student might not recognize as flutter waves because they don't produce the sawtooth pattern. The P waves' rate, approximately 360/min., gives them away as atrial flutter. This is also a good example of a constant 4:1 conduction, resulting in a regular QRS rhythm and regular pulse, at a rate of about 90/min. This demonstrates that not all narrow-complex rhythms between 60 and 100 bpm are "NSR". The low voltage in the limb leads makes this a good ECG to demonstrate that the flutter waves are regular and do not pause when the QRS happens, illustrating the separate actions of the atria and the ventricles. For students just learning 12-lead interpretation, this ECG serves to show that acute ST elevation M.I. is not the only valuable information that can be obtained from a 12-Lead, and that some leads are better than others for showing dysrhythmias.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
ATRIAL FLUTTER: Review of Clinical ECG Concepts
Dawn's January 19, 2013 Instructor Collection ECG is of Atrial Flutter with 4:1 AV Conduction. LOTS of important teaching concepts are conveyed by this tracing. These include:
Ken Grauer, MD www.kg-ekgpress.com [email protected]