
Submitted by jer5150 on Sat, 02/23/2013 - 21:36
Patient's clinical data: 55-year-old white man admitted to the surgical intensive care unit (SICU).
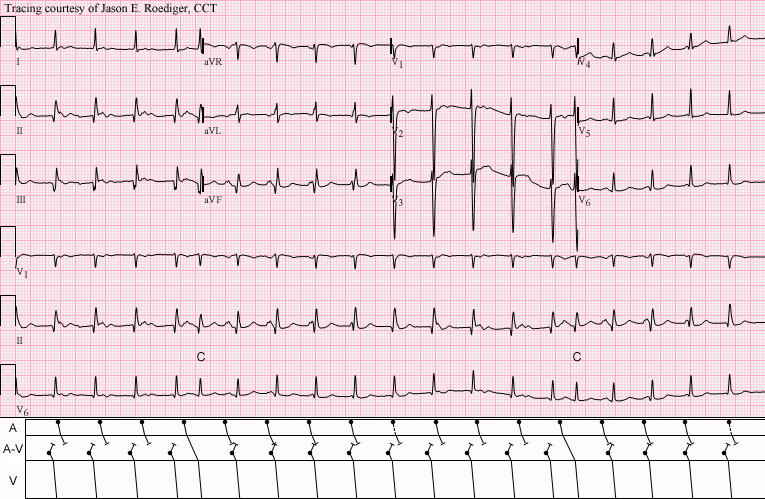
Part of the computer's interpretation was:
Sinus tachycardia 1st degree AV block Occasional
Premature supraventricular complexes
DO YOU AGREE WITH THE COMPUTER?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
AV junctional tachy with AV dissociation?
The computer's got it wrong again. I think the atria are under the control of the sinus node at a rate of 103bpm but there is a faster AV junctional tachycardia controlling the ventricles at a rate of 115bpm, producing AV dissociation. The AV dissociation isn't complete, however, and occasional sinus P waves fall in such a place that they can conduct to the ventricles and produce a capture beat. Theses are the 'premature' beats 5 and 15.
Dave R
AV Dissociation by Usurpation
GREAT tracing by Jason! I agree completely with Dave R's interpretation. This is AV dissociation by usurpation (ie, as per Dave - the slightly faster junctional rhythm takes over = "usurps" the pacemaking function despite underlying sinus tach). KEYS to recognizing this require the use of calipers (this being a perfect example of a rhythm you just can't interpret without using calipers! ).
Taking a final look at the tracing (to see if we might find a cause of this rhythm disturbance) - we see suggestion of prior inferior infaraction (large inferior Q waves) - but really no acute changes. So we have Sinus tach plus junctional tach resulting in AV dissociation by usurpation - the combination of which suggest Dig toxicity as the first clinical entity to rule out.
I'm sure Jason will elucidate further with a gorgeous laddergram! THANKS for posting this.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
INTERPRETATION
INTERPRETATION:1. Double tachycardia manifest in the form of . . .
2. . . . sinus tachycardia (rate about 107/min) dissociated from a slightly faster . . .
3. . . . idiojunctional tachycardia (rate about 115/min) and resulting . . .
4. . . . ventricular captures (C) with normal P-R intervals (5th and 15th beats; see laddergram).
5. Old inferior infarction of indeterminate age.
COMMENTS:
This is an example of dissociation due to usurpation. Critical lengthening of the R-P interval results in two ventricular captures which are recognized by shortening of the ventricular cycles and are just one of the six causes of early (i.e., premature) beats. Double tachycardia is usually associated with digitalis intoxication but that is unknown for this case.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]