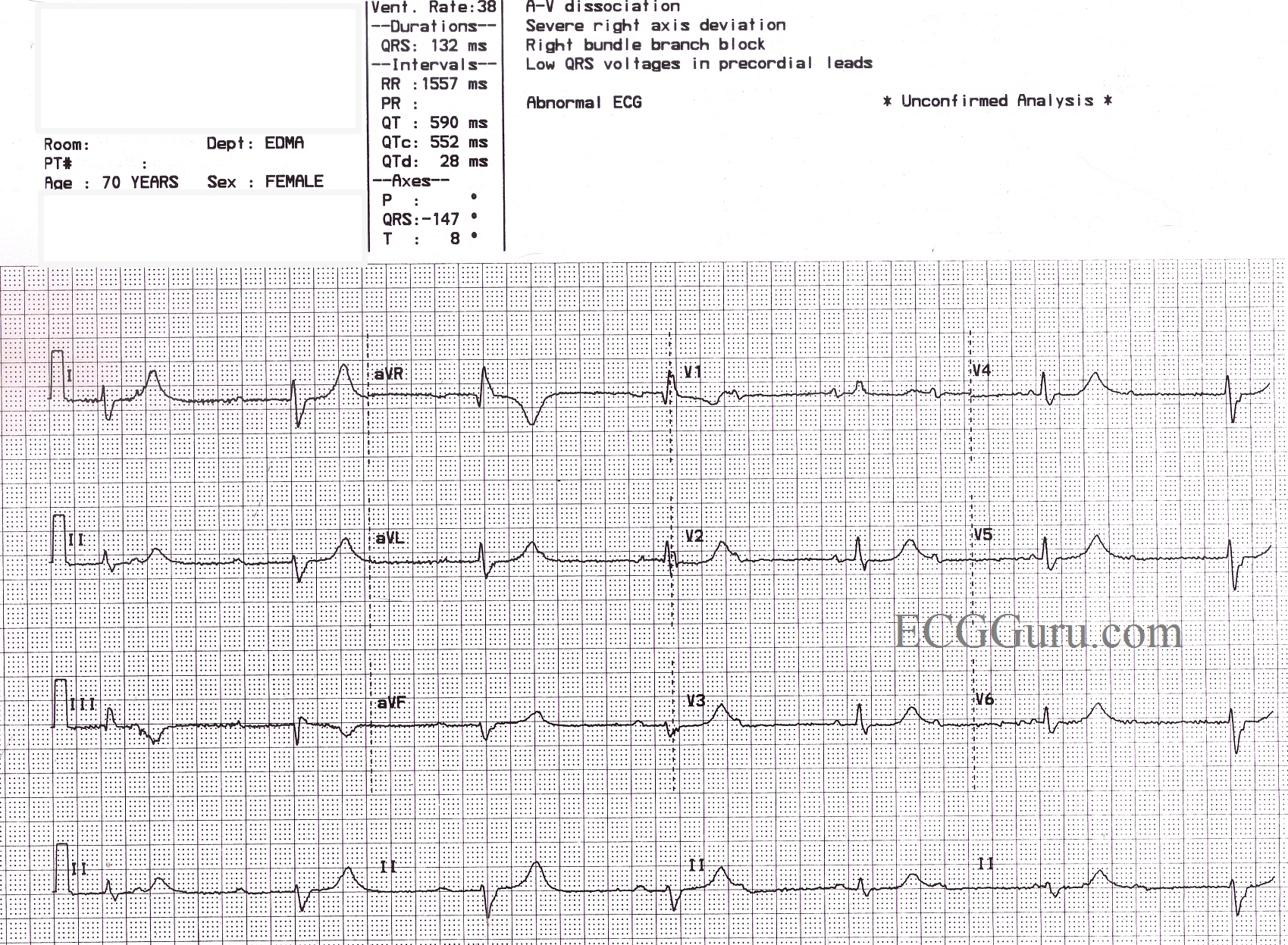
This ECG is from a 70 year old woman for which we have, unfortunately, no clinical information. It shows a sinus rhythm with a rate of about 72 bpm (NSR) with AV dissociation caused by third-degree heart block. The escape rhythm is junctional at a rate of 38 bpm. There appears to be a right bundle branch block, based on the QRS duration of 132 ms, and a wide S wave in Leads I and V6. The precordial leads do not show the usual RBBB pattern of rSR' in V1 and V2, and the r wave progression is poor (non-existent). This is felt to be due to poor lead placement (a good teaching point). Of interest, the ECG machine has reported a "severe right axis deviation" based on the tall upright R wave in aVR and the deep S in avF. In RBBB, the first part of the QRS represents left ventricular depolarization, and the terminal wave represents the delayed right ventricle. In effect, the two ventricles have their own electrical axes, which we can see because the ventricles are not depolarizing simultaneously. The axis of the LV appears to be normal in this tracing.
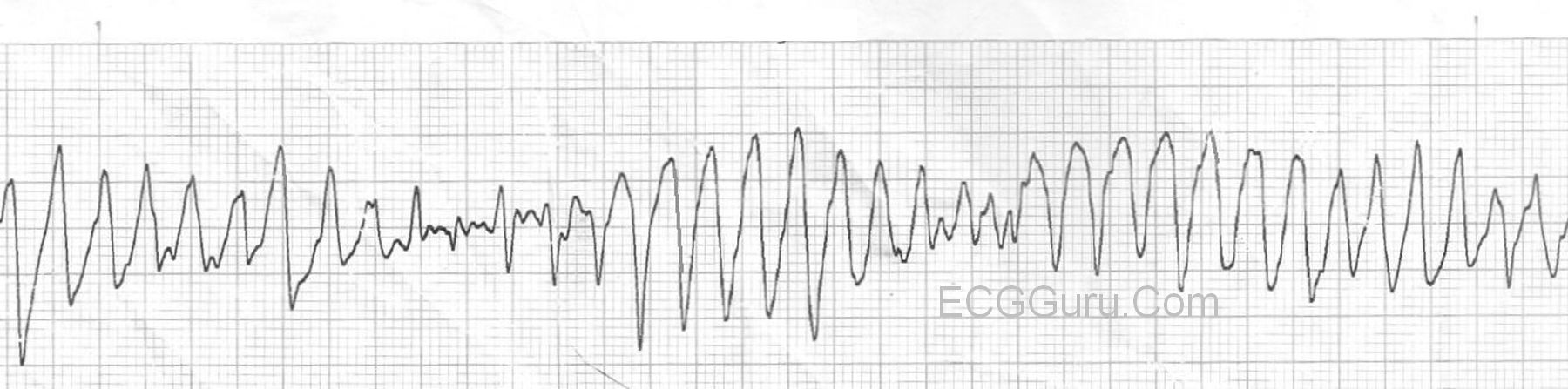
In addition to the above, this patient has a very prolonged QT interval. The QT is longer in bradycardic rhythms, but when corrected to a standard of 60 bpm (QTc), this patient's QT interval is still prolonged at QTc: 552 ms. Without clinical data, we cannot speculate as to why this patient's QTc is prolonged, but it can be a very dangerous situation. Follow the links for more information on QT prolongation and Torsades de Pointes and Long QT Syndrome.
As always, we welcome comments from our members adding insight to this interesting ECG, and also questions you would like to ask our Guru members.