The Patient This ECG was obtained from a 51-year-old man who presented to EMS with acute chest pain. He had a history of hypertension, 40 pack-year smoker.
Hospital Course He was diagnosed with anterior wall STEMI and taken to the cath lab. He was rated Killips Class 1 (no evidence of congestive heart failure), TIMI risk score 4 (14% risk of all-cause 30-day mortality). He underwent primary percutaneous coronary intervention (PCI) of the proximal left anterior descending coronary artery (LAD).
Ten days post PCI, the patient had ventricular arrhythmias and went into cardiac arrest, but was resuscitated. He continued to have occurrences of non-sustained ventricular tachycardia (VT), progressing to sustained VT. Electrolytes were monitored and corrected when necessary. The patient expired before any further diagnosis was made.
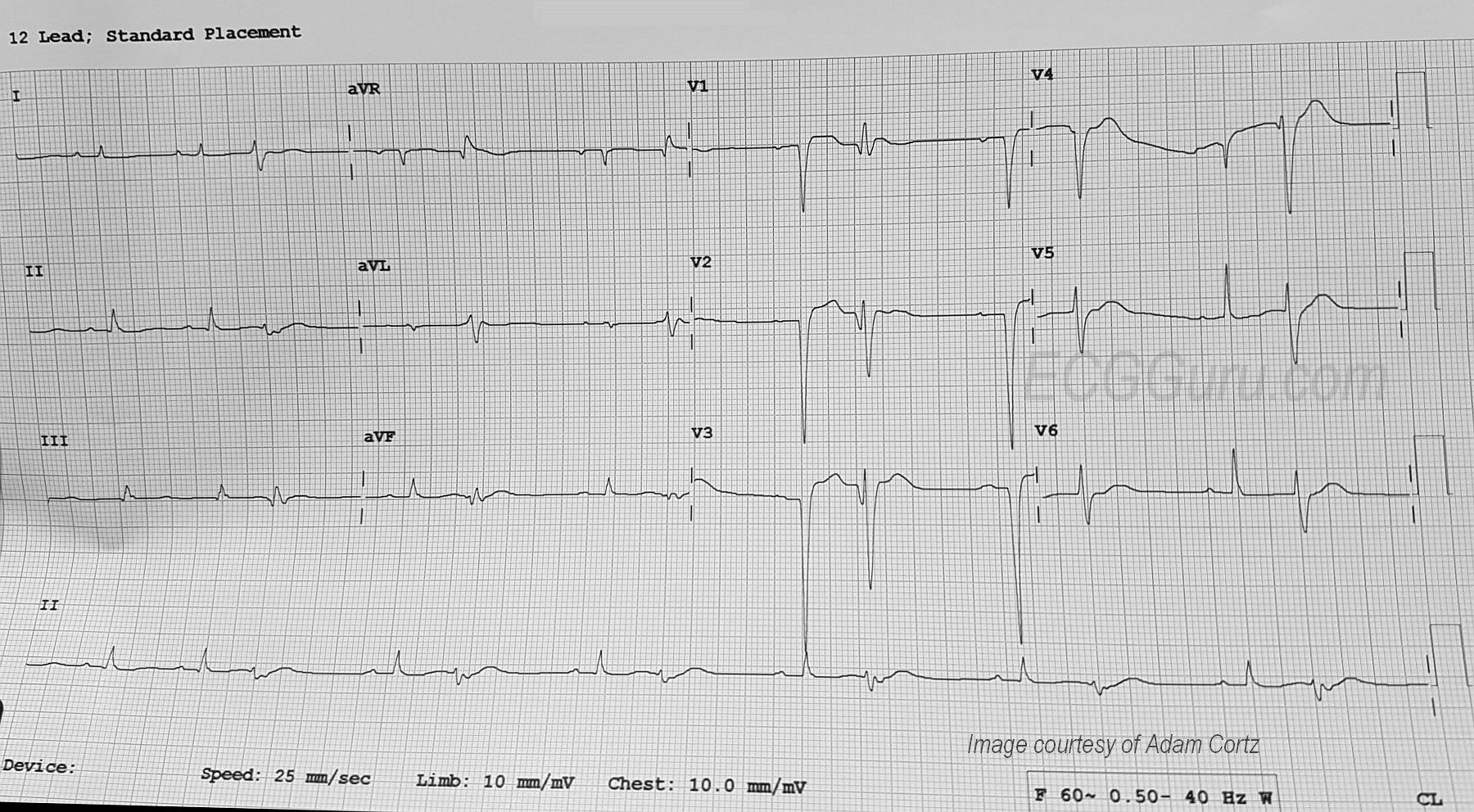
ECG Interpretation The rhythm is sinus at a rate of about 80 bpm (first two beats). The PR interval is about .18 seconds. The QRS duration is about .10 seconds. After the second sinus beat, ventricular bigeminy occurs. Every other sinus beat is obscured by the PVCs. By the end of the strip, the underlying sinus rhythm has slowed slightly.
The ECG signs that the ectopic beats are ventricular are: lack of P waves associated with the premature beats, QRS width about .16 seconds, and compensatory pauses. The axis of the sinus beats is around 60 degrees (normal), but the axis of the premature beats is difficult to determine due to the low voltage and biphasic QRS complexes in the frontal plane leads. It is also difficult to determine ST and T wave changes in the PVCs for the same reason.