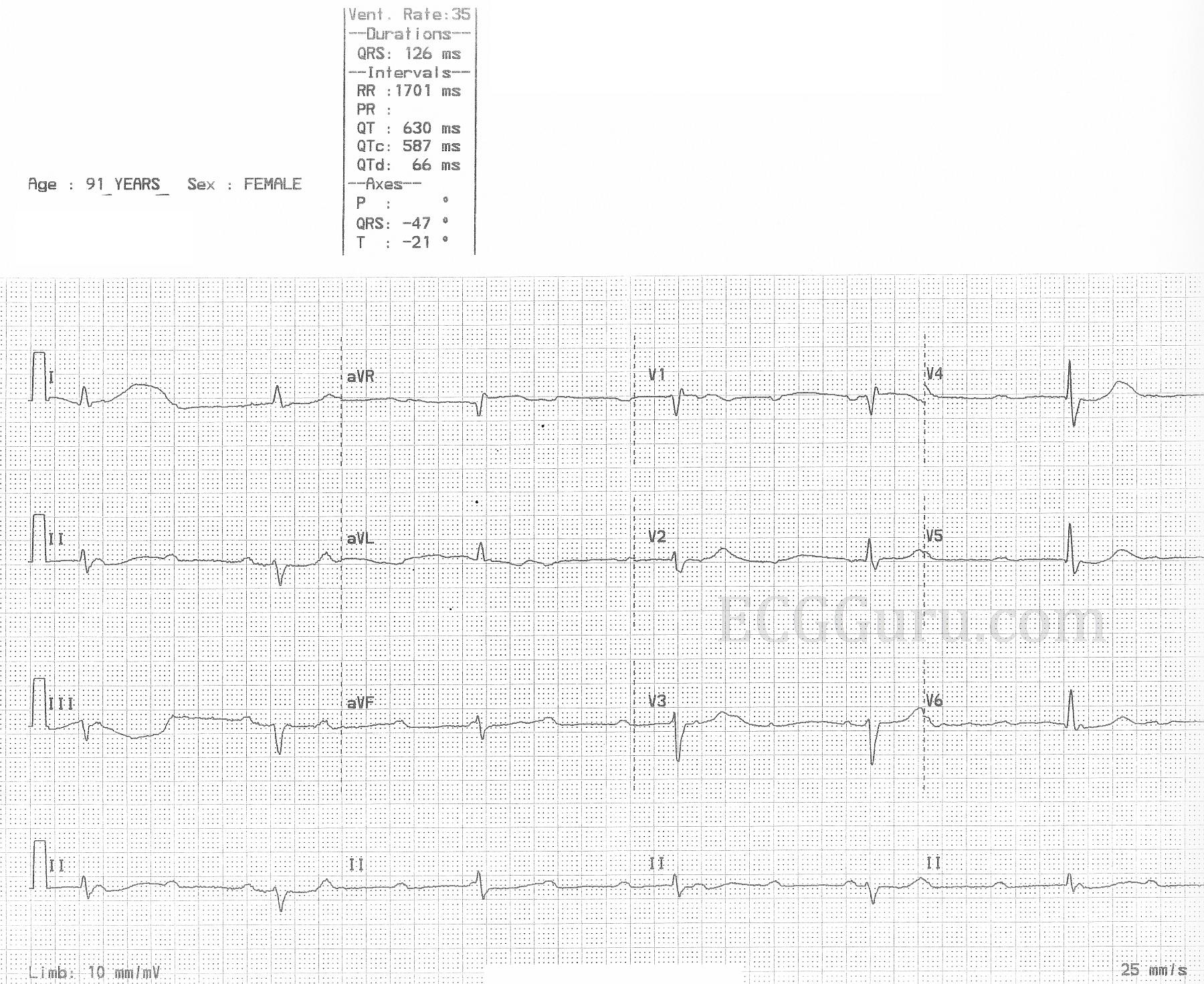
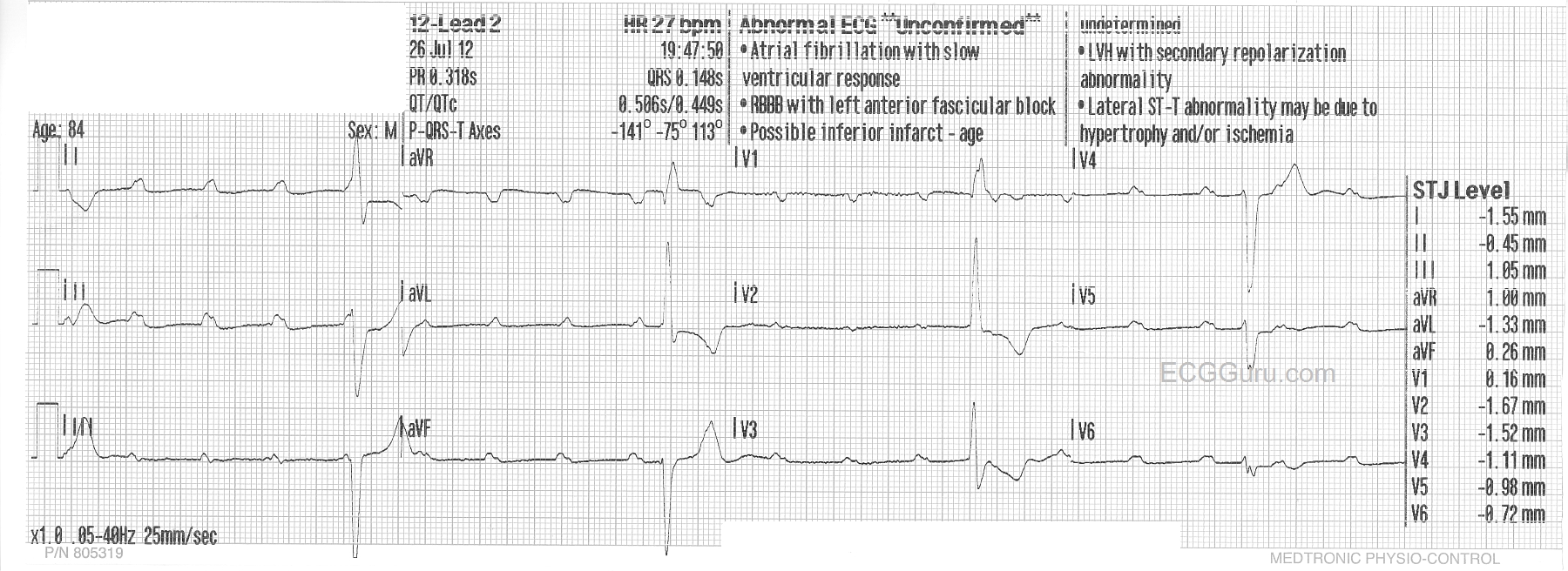
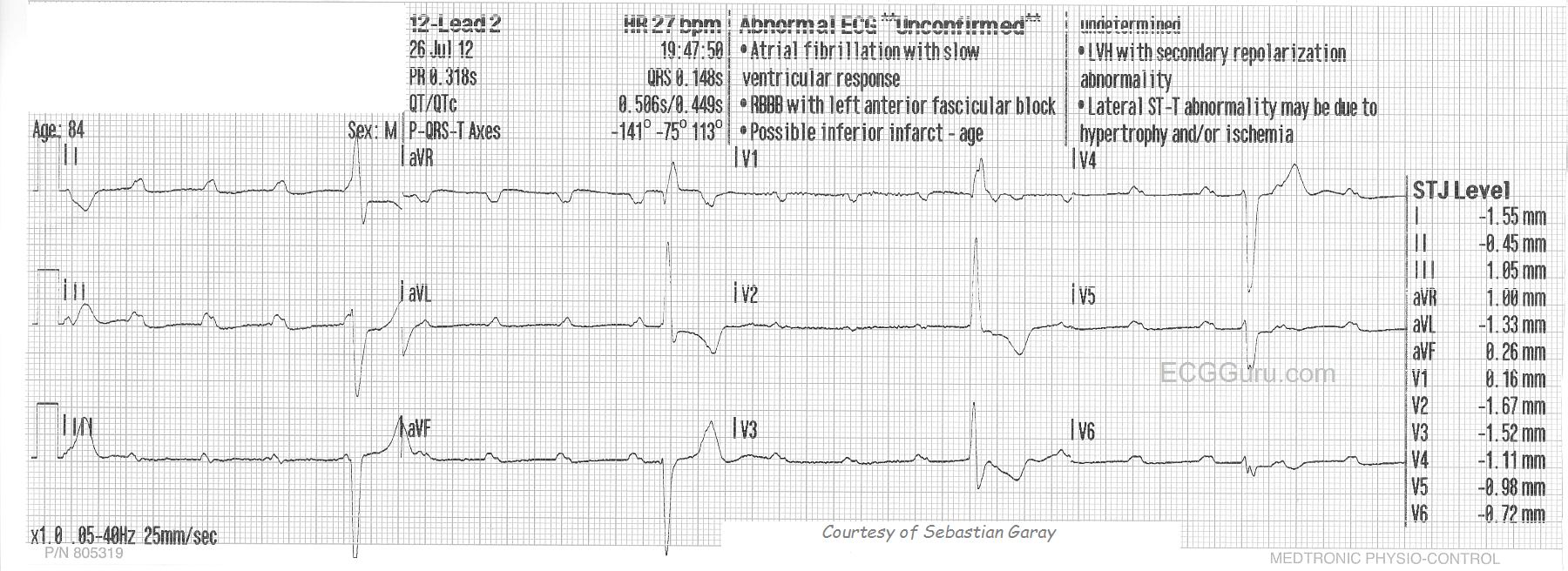
This ECG is taken from a woman who had suffered for several years with intractable intermittent atrial fibrillation. She had tolerated medications poorly, and several attempts at electric cardioversion had resulted in only temporary relief. Ultimately, she chose to undergo AV node ablation. In the electrophysiology lab, her AV node was destroyed, preventing the atrial fib impulses from penetrating into the ventricles. This resulted in a “man-made” complete AV block. A pacemaker was implanted in the EP lab. When she is in atrial fibrillation, the fibrillatory waves of the atria INHIBIT the atrial pacing electrode from firing, so she has no paced P waves at that time. The right ventricular pacing electrode functions without inhibition, and makes a wide QRS complex with a leftward axis deviation (normal for RV pacing).
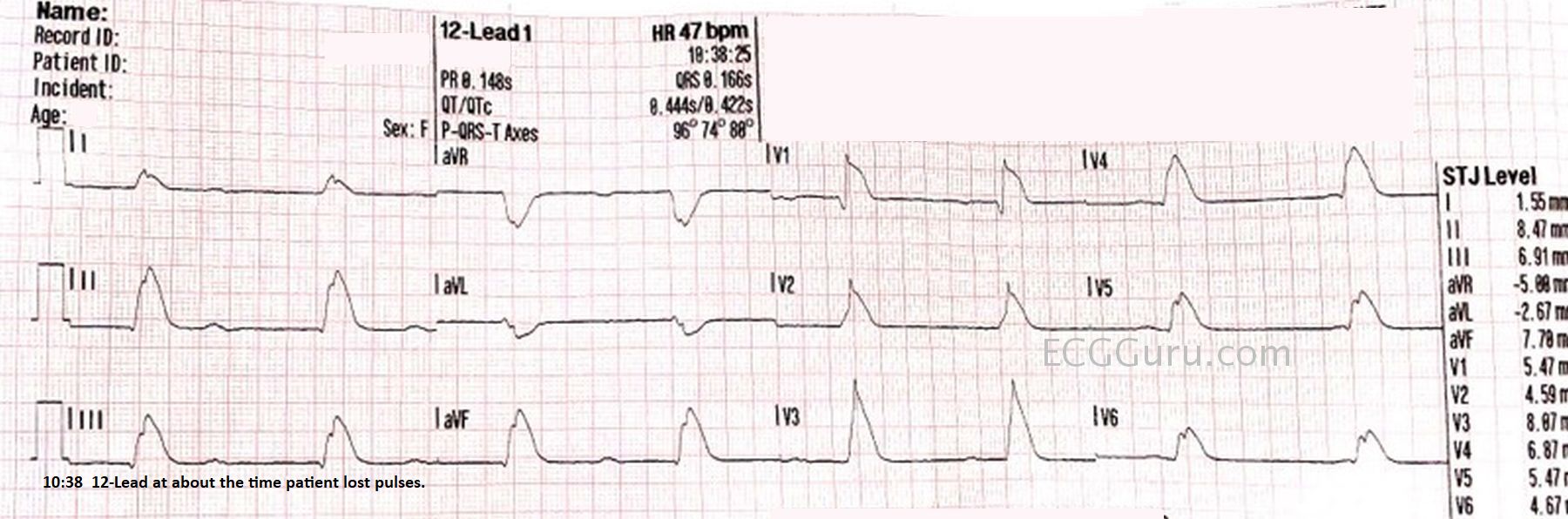
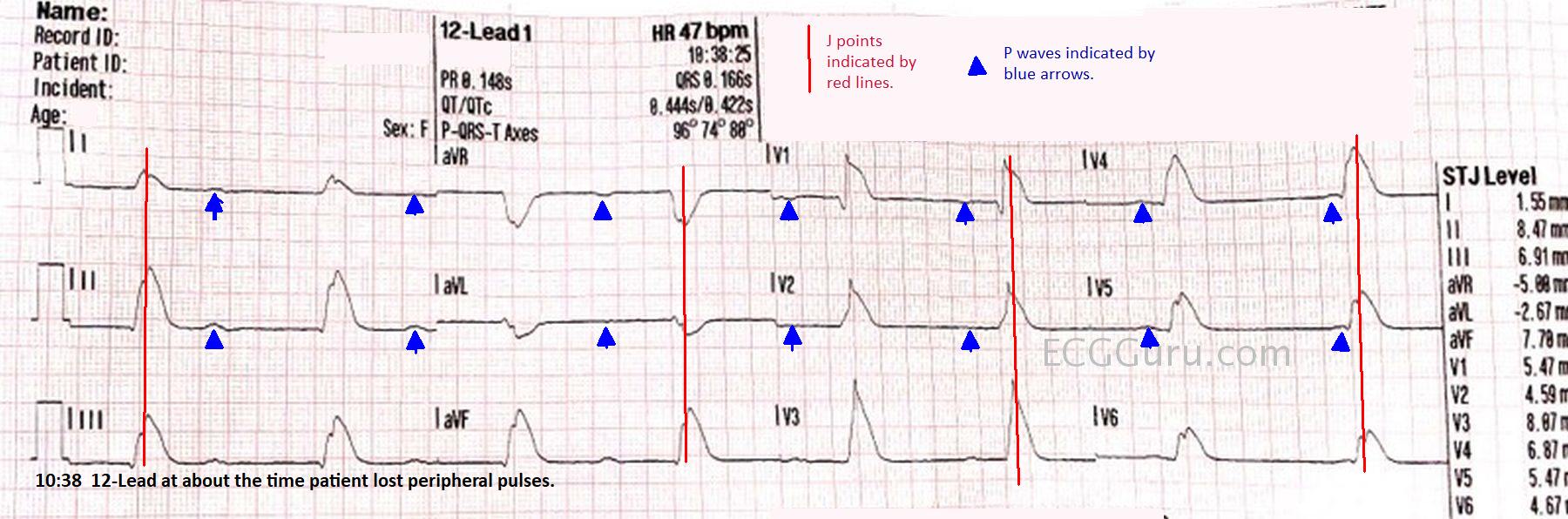
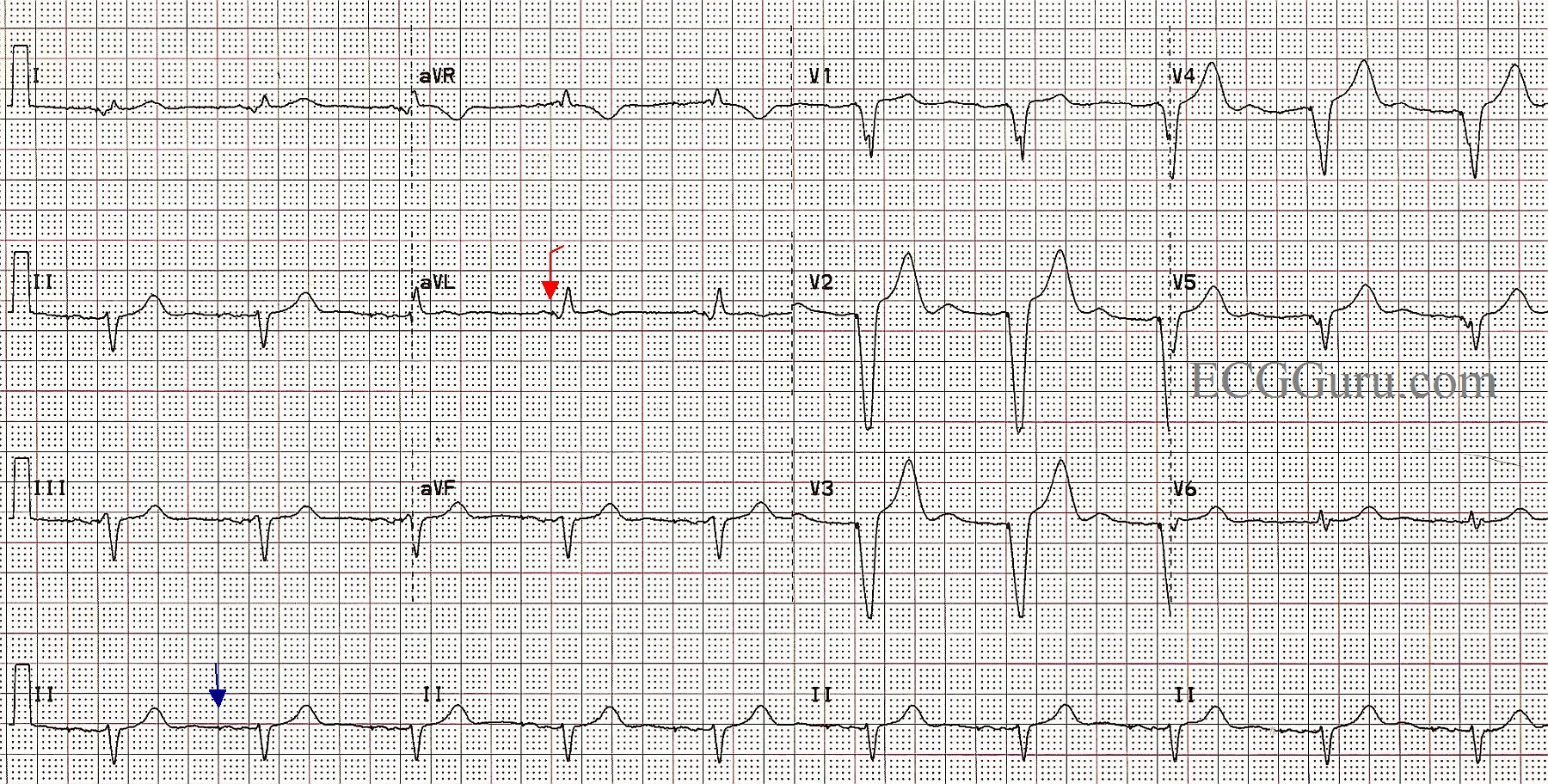
In this ECG, we see the patient WITHOUT atrial fib, and the pacemaker is pacing the atria AND the ventricles, in a sequential fashion. The spikes are very hard to see, as this is a “bipolar” pacemaker, which makes much smaller spikes than a “unipolar” pacemaker. Some ECG machines will automatically enhance the spikes, but this one did not. We have marked a “sample” atrial spike in blue for you and one of the ventricular spikes in red. Each beat on this ECG actually has appropriately-timed atrial and ventricular stimuli (spikes), and the patient has optimized cardiac output provided by the “atrial kick”. A P wave occurring just before a QRS indicates that the ventricles are filling from the forceful contraction of the atria. This provides much better filling than when the atria are not beating or are fibrillating.
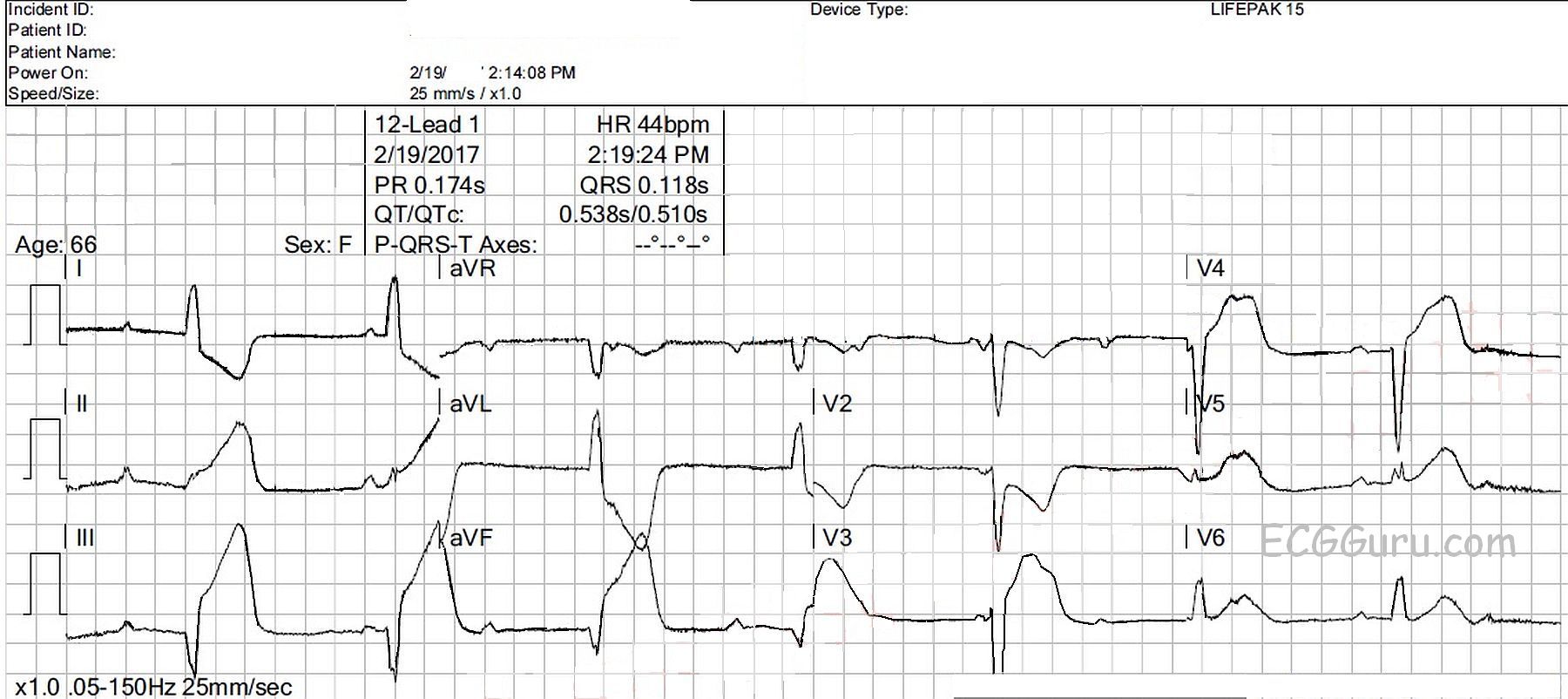
This is a good ECG to use to show your students how we can recognize a paced rhythm without being sure of the spikes. Of course, without other evidence (patient history and exam), we can’t know for sure that this is a paced rhythm, but the steady, normal rate, wide complexes, and left axis deviation are signs of RV pacing. Look for negatively-deflected QRS complexes in II, III, and aVF and positive QRSs in aVL and aVR.
When pacing only one ventricle, the impulse travels relatively slowly through the other ventricle, resulting in wide QRS complexes. This then results in SECONDARY ST-T WAVE CHANGES. Wherever the QRS is positive, you will normally see some ST depression and T wave inversion. In leads with negative QRS complexes, the opposite is true, and you will see ST elevation and upright T waves. This can make evaluation of ST segments for acute M.I. difficult.