This series of ECGs was taken during ambulance transport of a 67 year old man with chest pain. Earlier the same week, this man had been discharged from the hospital after having a cardiac cath, angioplasty, and stents. He was discharged the next day. The patient stated that, until that hospital admission, he was healthy, athletic, and had no significant medical history. He is currently taking a statin, atenolol, and "one of the new blood thinners" - he didn't know the name.
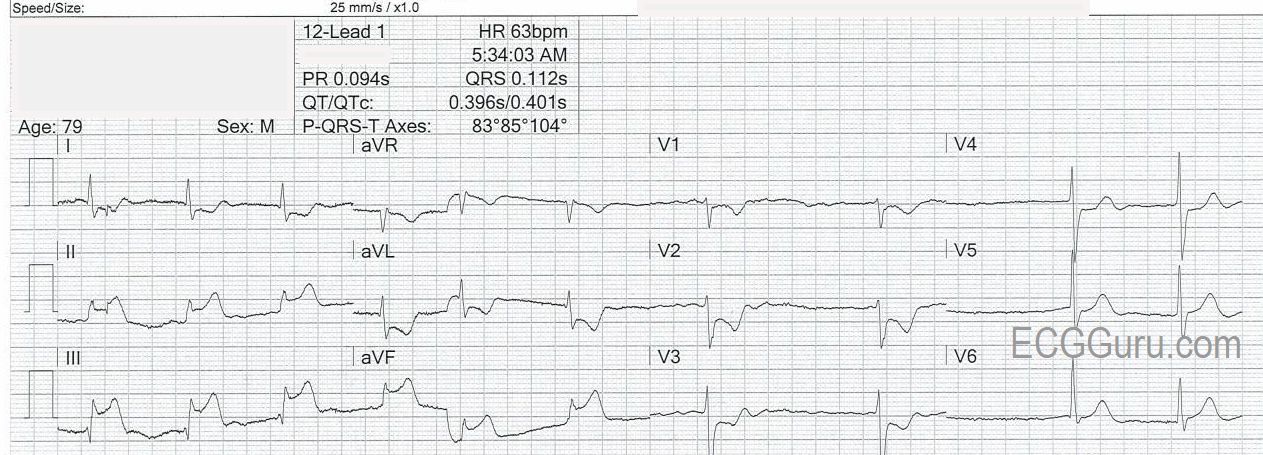
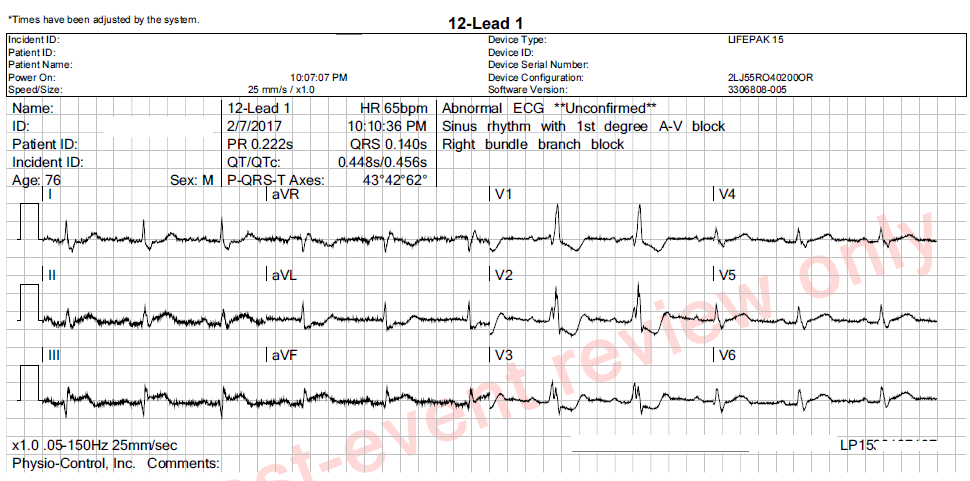
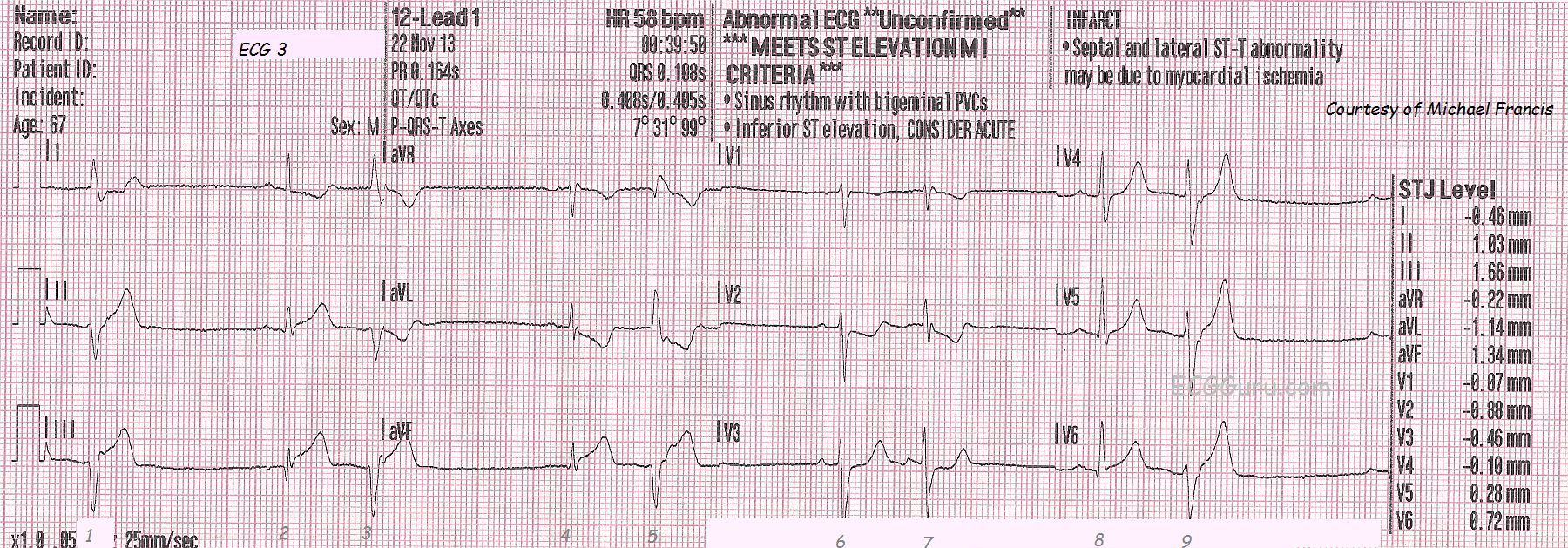
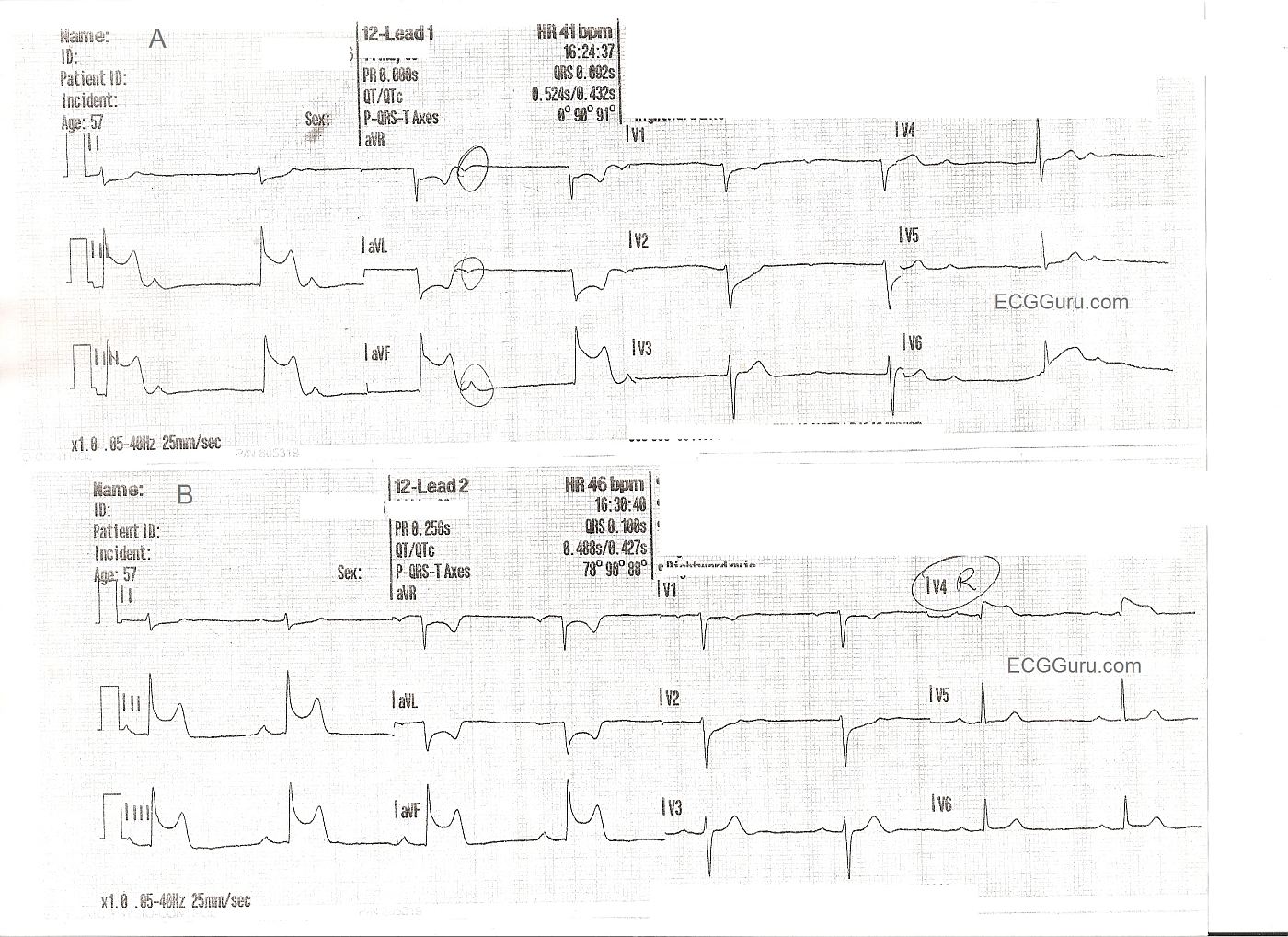
ECG No. 3 is the first one shown here, taken at almost 39 minutes after midnight. The patient was complaining of chest pain of 8 on a 1-10 scale. His skin was pale, cool, and clammy. The ECG shows acute inferior-posterior M.I., with ST elevation in II, III, and aVF and reciprocal ST depression in V2, and V3. V1 would normally be depressed in posterior extension of an inferior wall M.I. - unless the right ventricle is also infarcted. The message from the right ventricle to V1 would be "elevate", countering the message from the posterior wall, "depress". The rhythm is sinus with ventricular bigeminy. The rescue crew notified the hospital of a "STEMI Alert". The patient received I.V., O2, nitroglycerin spray and paste, as well as aspirin. The patient's BP was 144/92.
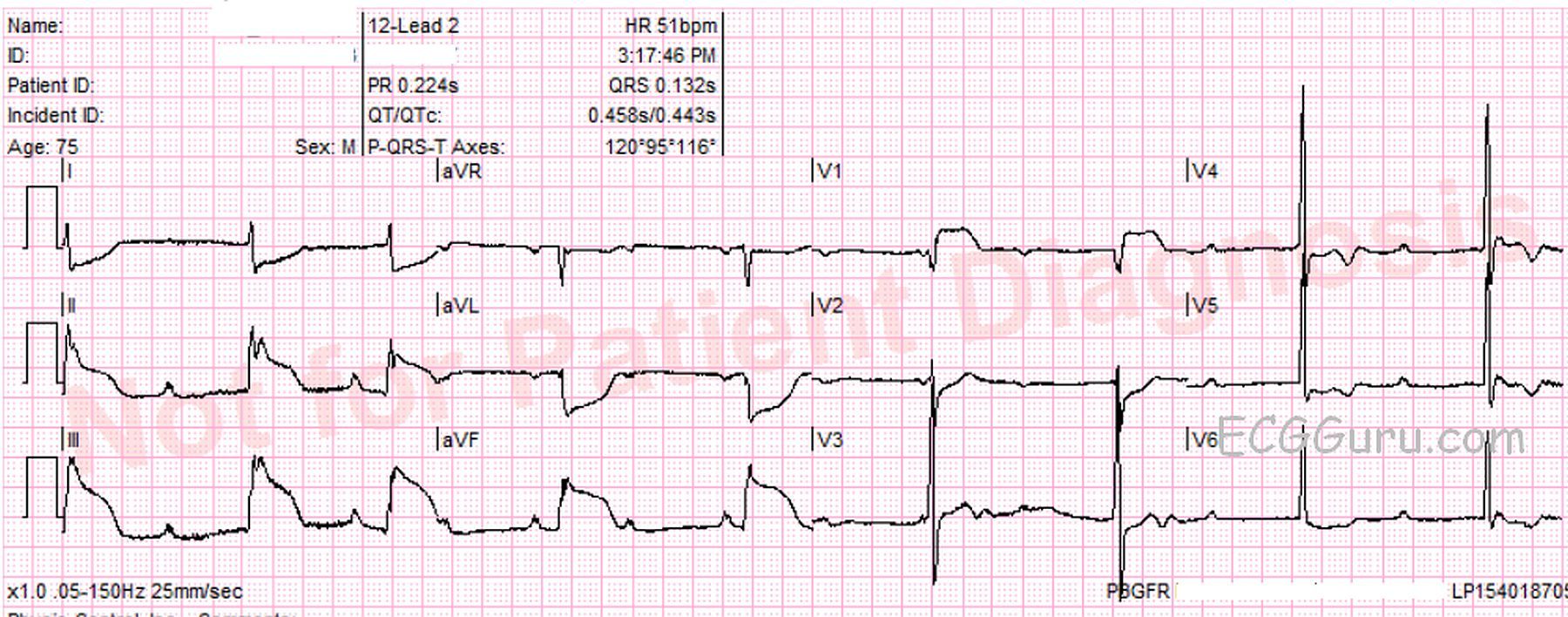
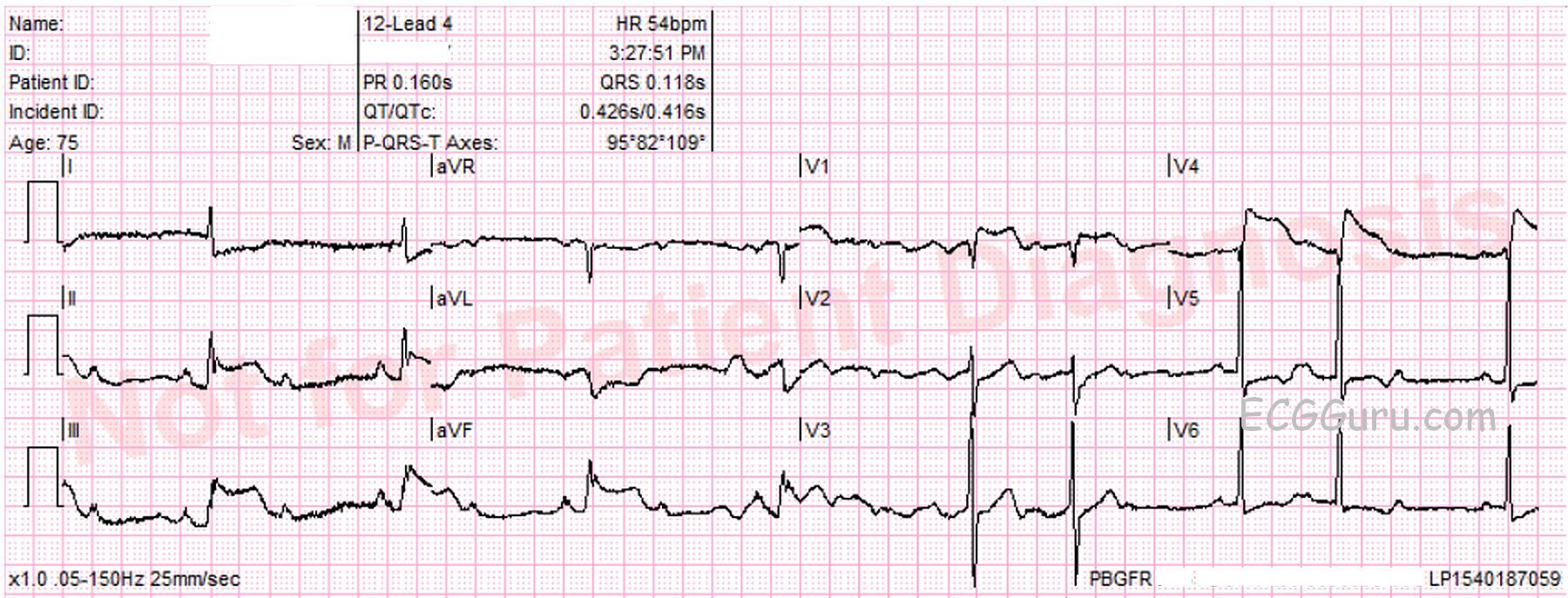
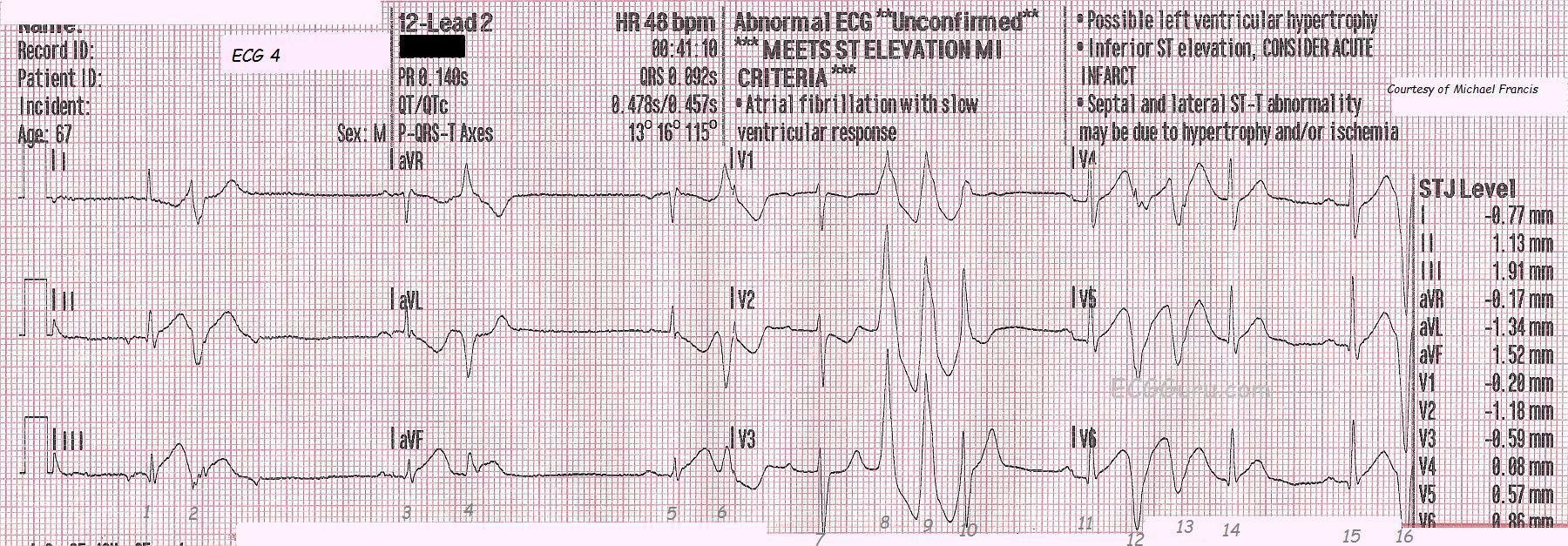
ECG No. 4 was taken at 12:41 a.m. It shows a change in P waves probably reflecting a low atrial focus. The patient has a slow underlying rhythm with ventricular bigeminy that is probably multifocal. It is very hard to determine multifocal PVCs when there is no concurrent rhythm strip, but this is a three-channel ECG machine, and the rhythm strips are run separately from the 12-lead. There are runs of V Tach toward the end of the ECG, and this is not a good sign in a patient with ST elevation. In some cases, the V Tach can become persistent, in others it is transient. The ST elevation and reciprocal depressions are still evident.
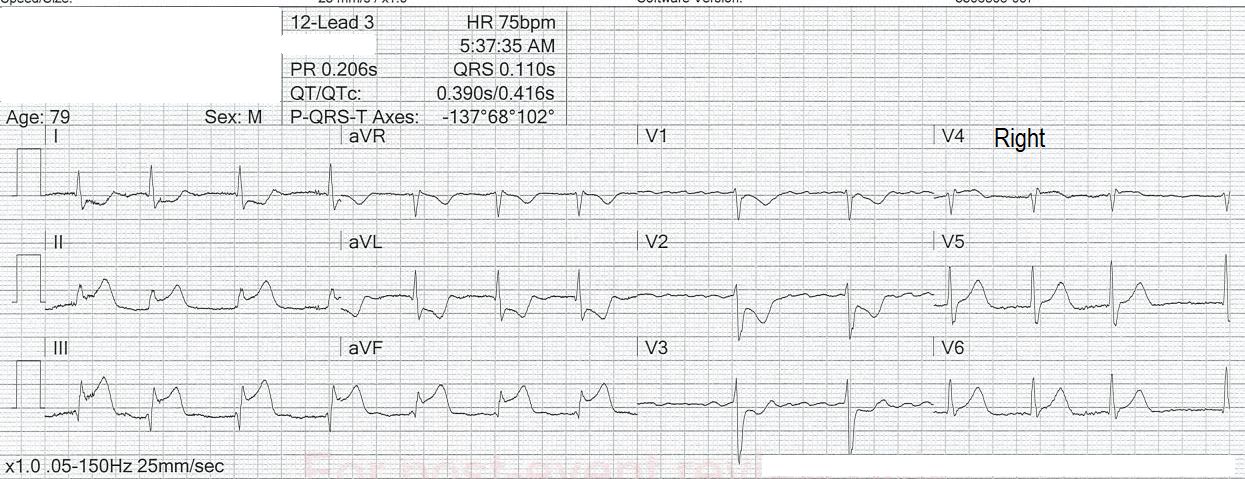
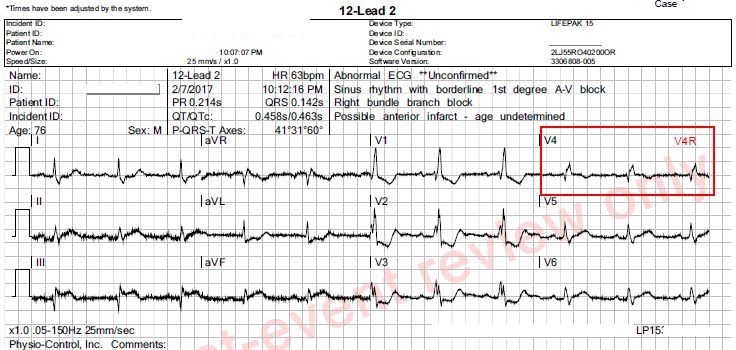
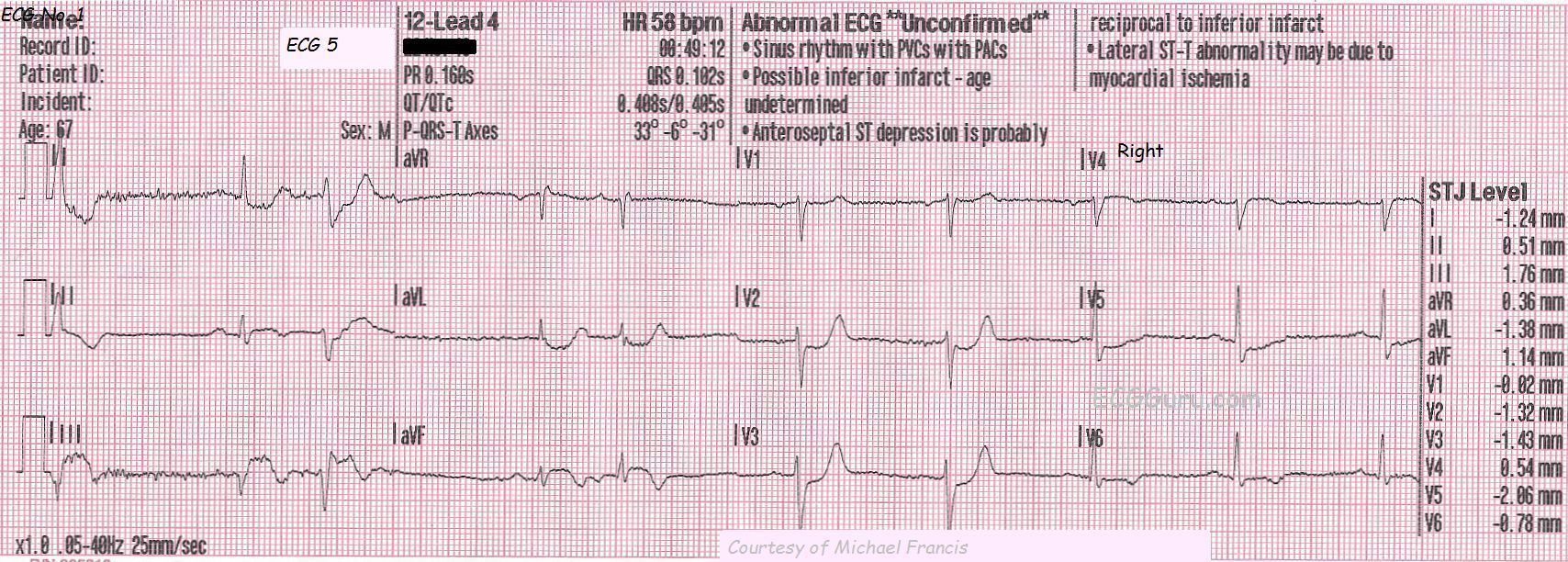
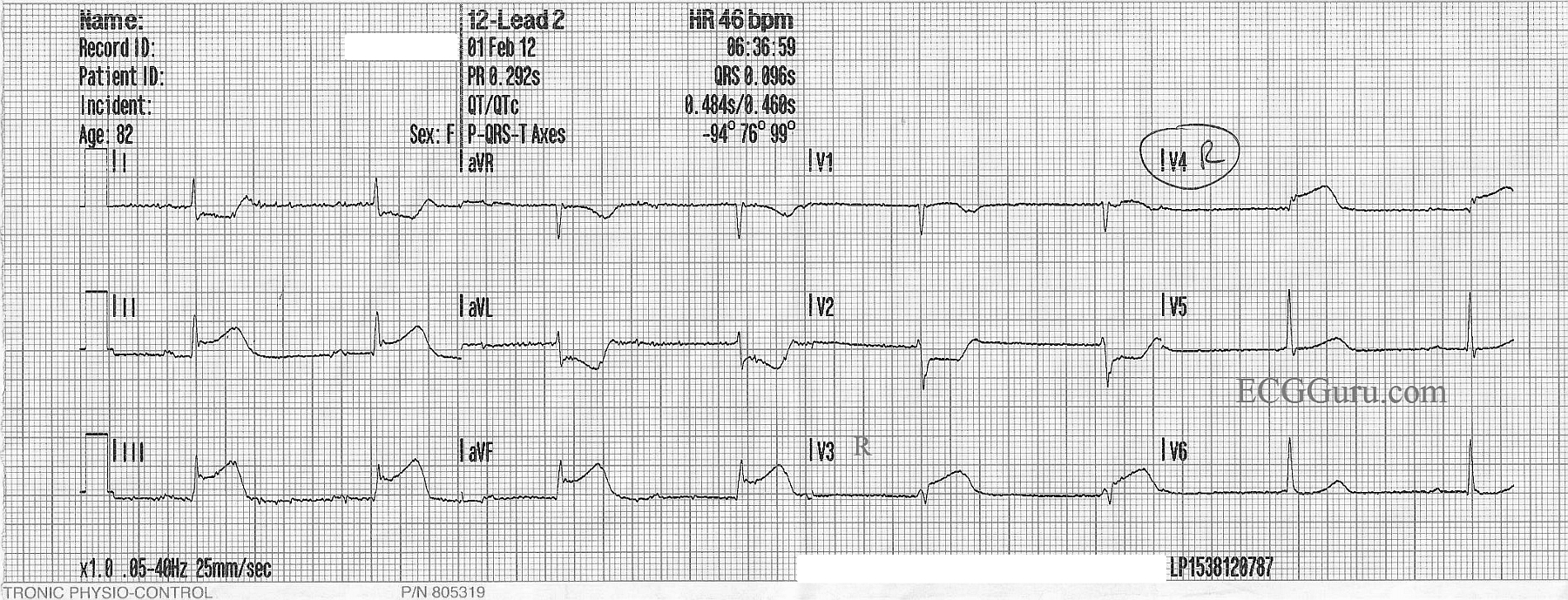
ECG No. 5, taken at 12:49 a.m., shows further development of the ST segments, and the classic "domed" shape of STEMI. In addition, a pathological Q wave has appeared in Lead III, possibly indicating permanent damage from this M.I. In this ECG, the paramedics have moved the V4 wire to the V4 Right position to better view the right ventricle. V4 Right is slightly elevated, and definitely dome-shaped, like a frown. This is an indication that the RV is injured, and medications that lower BP (especially nitroglycerin) should be avoided in the pre-hospital setting because of the danger of loss of preload of the RV and sudden drop in cardiac output. The patient's BP at this time was 138/85.