Years ago, I was tasked with introducing 12-lead ECG interpretation to firefighter/paramedics who had been using ECG for rhythm monitoring for years. Some were eager to add to their skills, others - not so much. The feeling was, we have been doing just fine as we are. When finally convinced that they could interpret STEMI with a 12-lead, many were content to use the 12-lead ECG only for that.
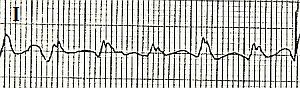
To illustrate to students the great value of multi-lead assessment, I devised a little "quiz". I showed the students ten to twelve short rhythm strips, like you see here. All were cropped from 12-lead ECGs. I asked my class to interpret the strips as they would if they were taking an ACLS class. Usually, all did fine, or so they thought. When shown the 12-lead ECGs the strips were taken from, EVERY student changed his or her mind on EVERY ECG. The lesson is: sometimes what we are looking for shows up in some leads and not others. You can find this illustrated hundreds of times just in the ECG archives on this site. I will supply some ECGs here on this page over the next few weeks that you could use to show your own students the value of "multi-lead assessment".
What started as a hard-sell turned out to be a fun exercise.
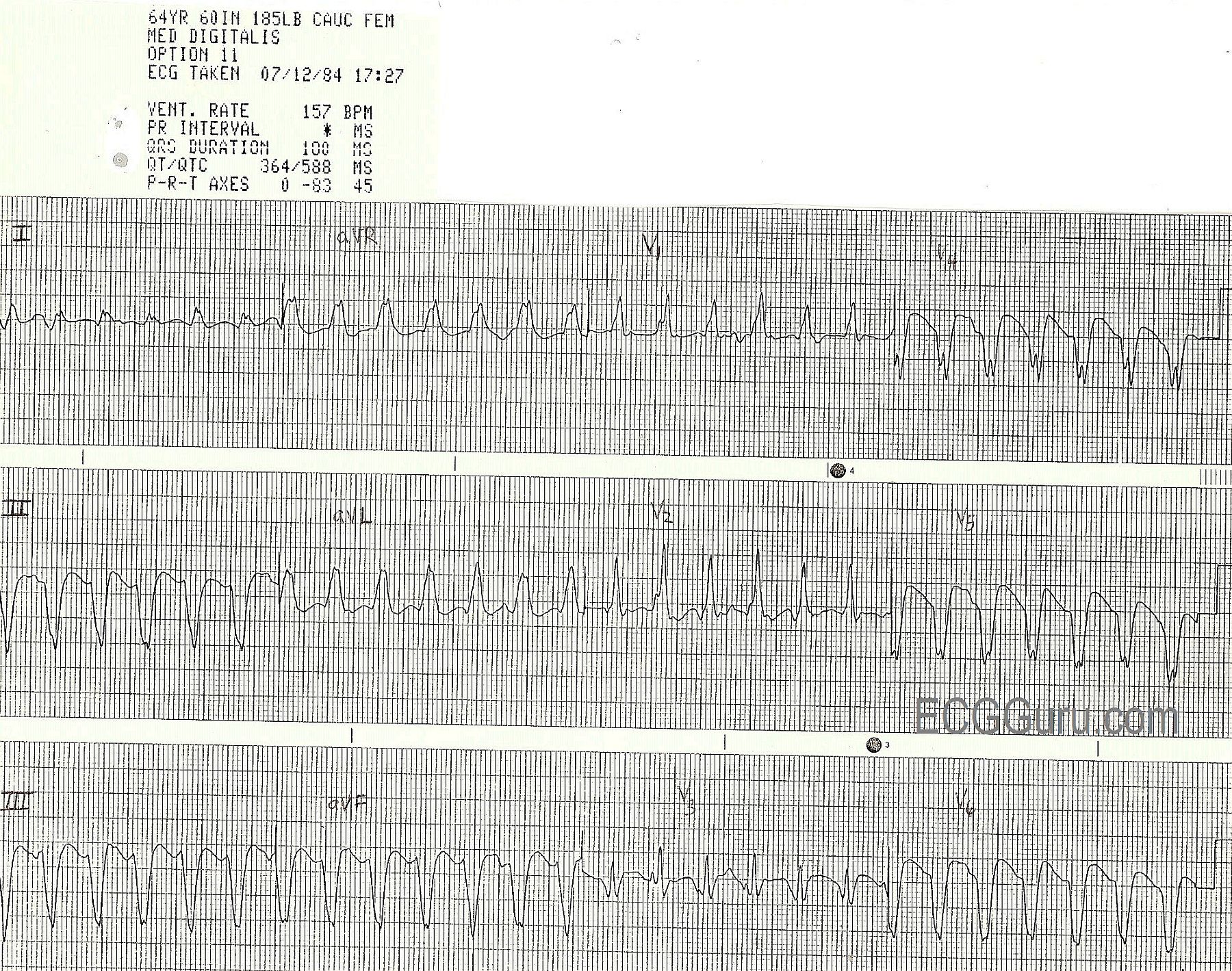
The ECG shown here is of a patient in V Tach. There are several strong signs that this is V Tach, including the wide QRS complexes, lack of associated P waves, "backward" axis, also called extreme right axis deviation (Leads II, III, and aVF are all negative and aVR is positive), and V6 is negative. For more review of the differential diagnosis of wide-complex tachycardias, go to our Ask the Expert answer from Jason Roediger. This LINK willl take you to Dr. Grauer's informative webpage where he offers a step-by-step guide to differentiating the WCTs.
The focus of THIS lesson is that, while the patient is in V Tach, and it is in every lead, the tell-tale signs are harder to see in some leads than others. Remember to show your Remember to share with your students that the channels of the ECG (in this case three) are run simultaneously, so that the same heartbeat is seen several times - once for each channel.