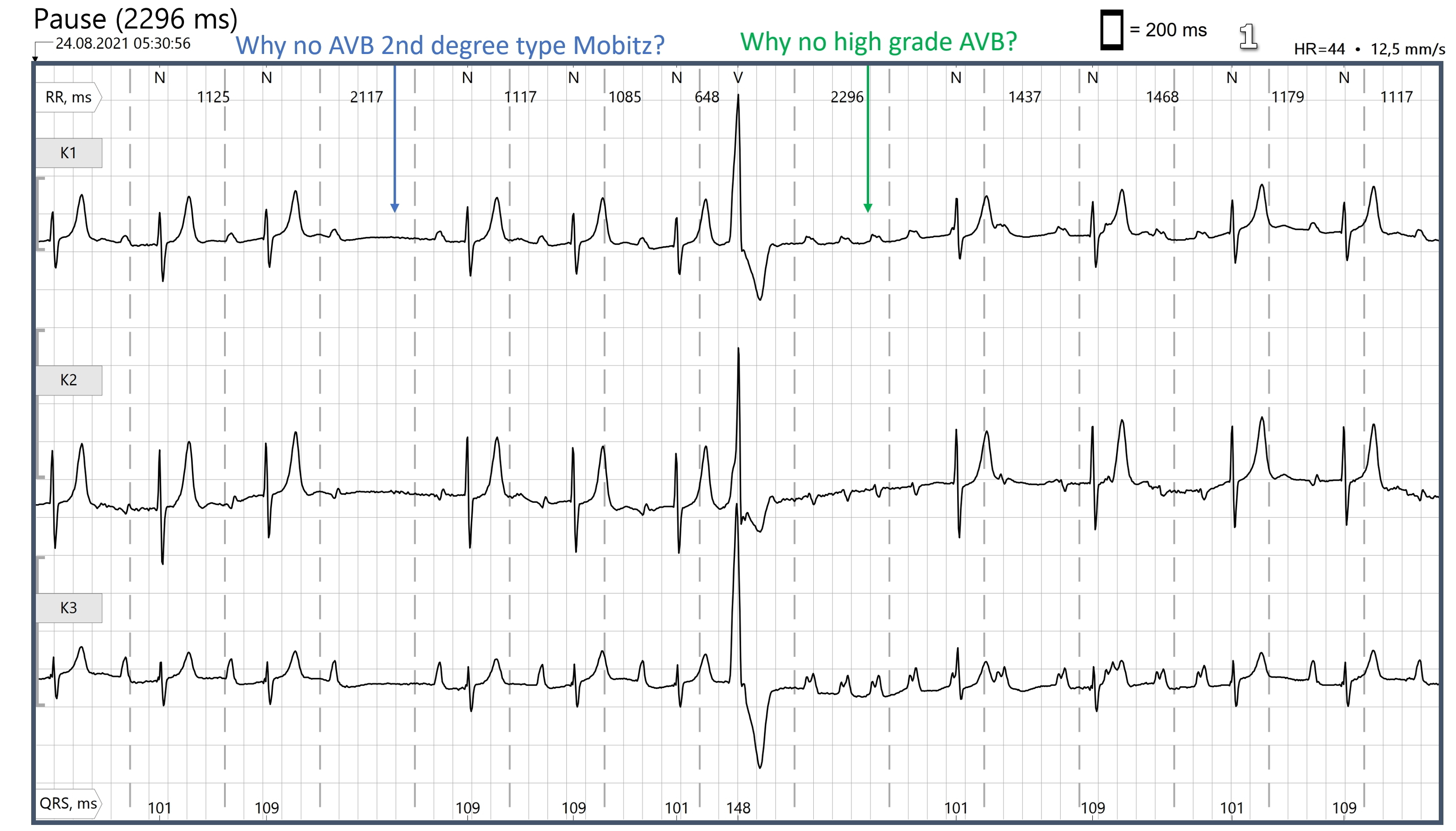
Second-degree AV block can either be Type I (Wenckebach) or Type II. In either case, some P waves are conducted to the ventricles, and some are not. Type I blocks usually occur in the AV node, and are often benign. Type II blocks are more often "sub-Hisian", or fascicular blocks, and are more likely to progress to higher levels of AV block and bradycardia. When a second-degree AVB is conducted in a 2:1 ratio, it is difficult to differentiate Type I from Type II. Features that favor the diagnosis of Type I are narrow QRS complex and the non-conducted P waves land on the previous T waves - during the refractory period of the ventricles.
Type II blocks are more likely to have a wide QRS with a bundle branch block morphology. That is because Type II blocks often reflect serious fascicular disease. A typical Type II block is a persistent bifascicular block (ex: RBBB and left anterior hemiblock)) with an intermittent block in the third fascicle. Another way to think of it is an intermittent tri-fascicular block. If that one remaining fascicle stops conducting, the patient will be in complete heart block.
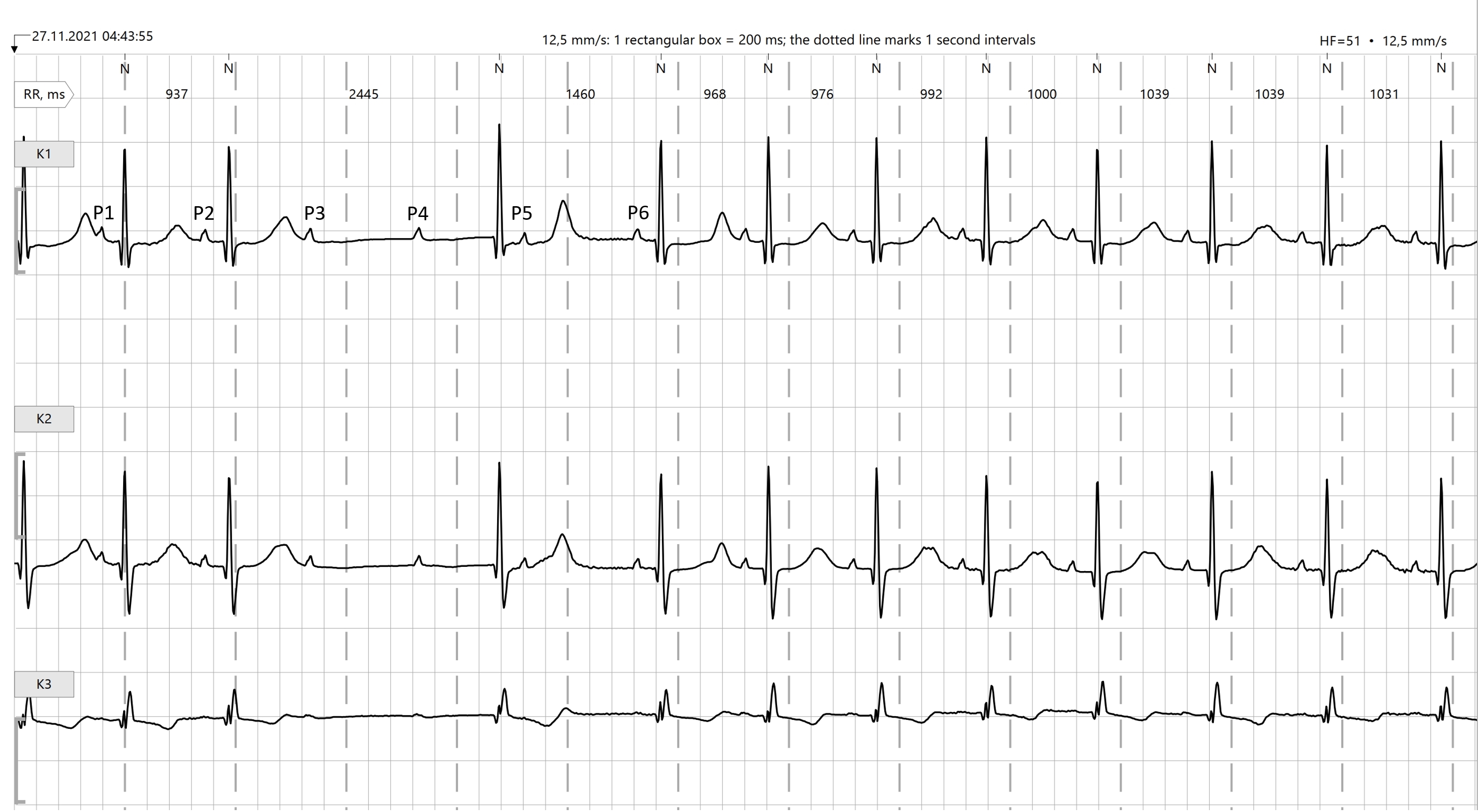
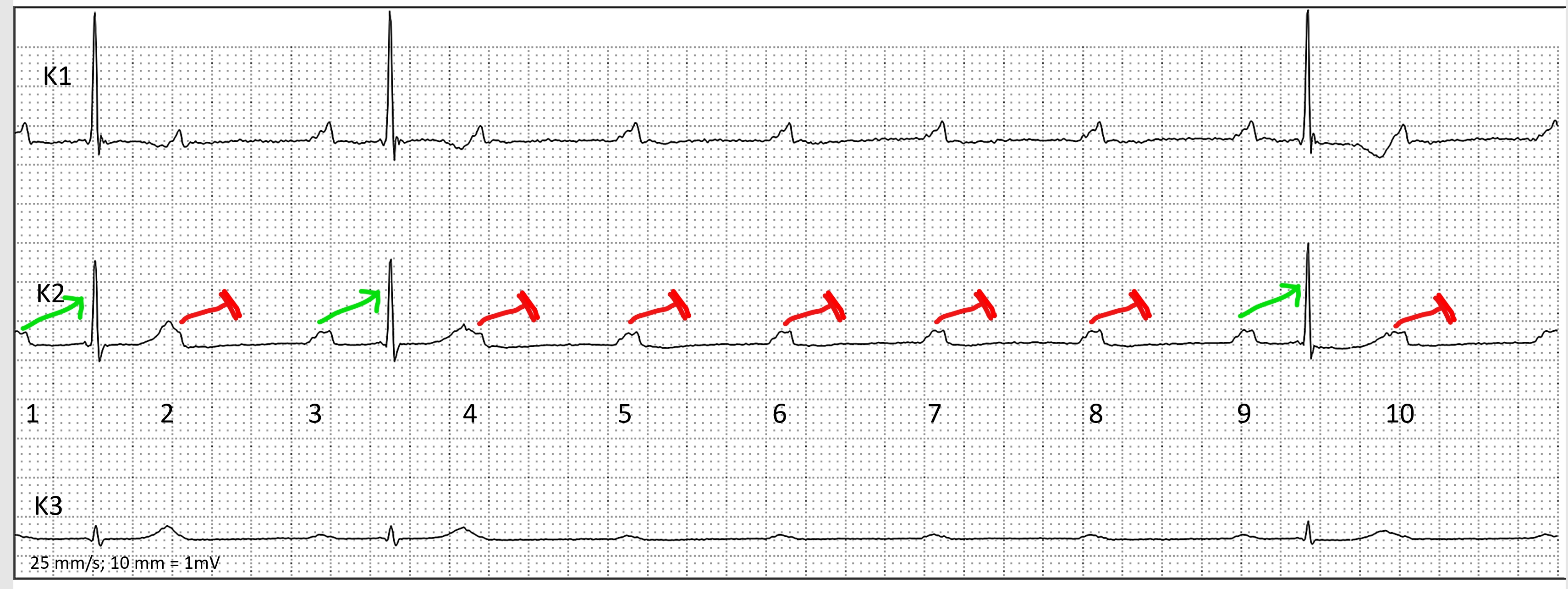
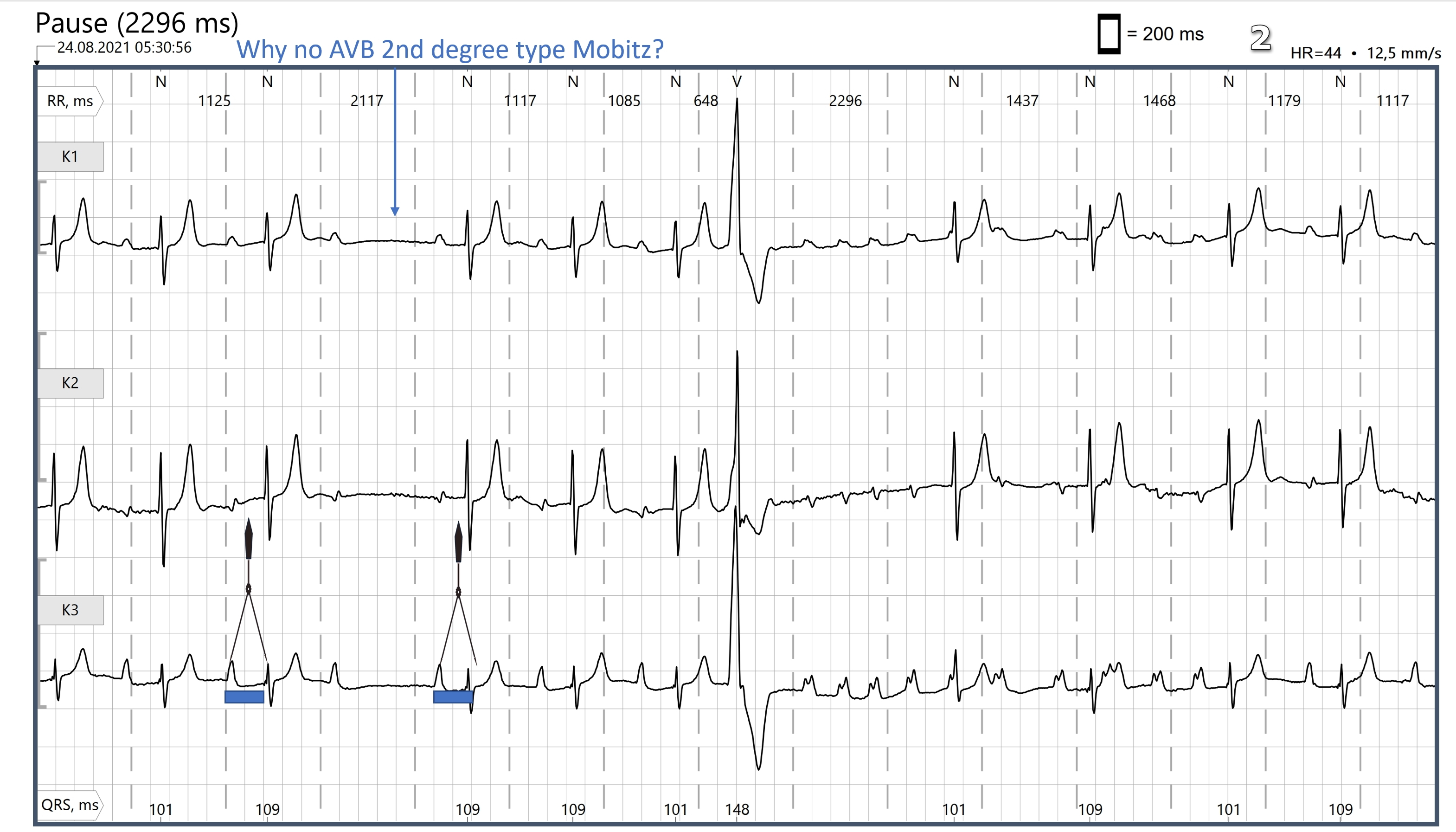
Signs of Type II blocks include the wide QRS and also two or more non-conducted P waves in a row. Also, P waves that are "out in the open", away from the refractory period, but fail to conduct are an ominous sign.
One strategy for reacting to a 2:1 block is to first assess the ventricular rate (54 bpm in this example). Determine if it is adequate for the patient's hemodynamic stability. If not, act to increase the rate. Otherwise, it may be prudent in the stable patient to watch the rhythm strips for a while. Sometimes, two p waves in a row will conduct - unmasking either progressive prolongation of the PR interval (Type I) or stable PR intervals (Type II).
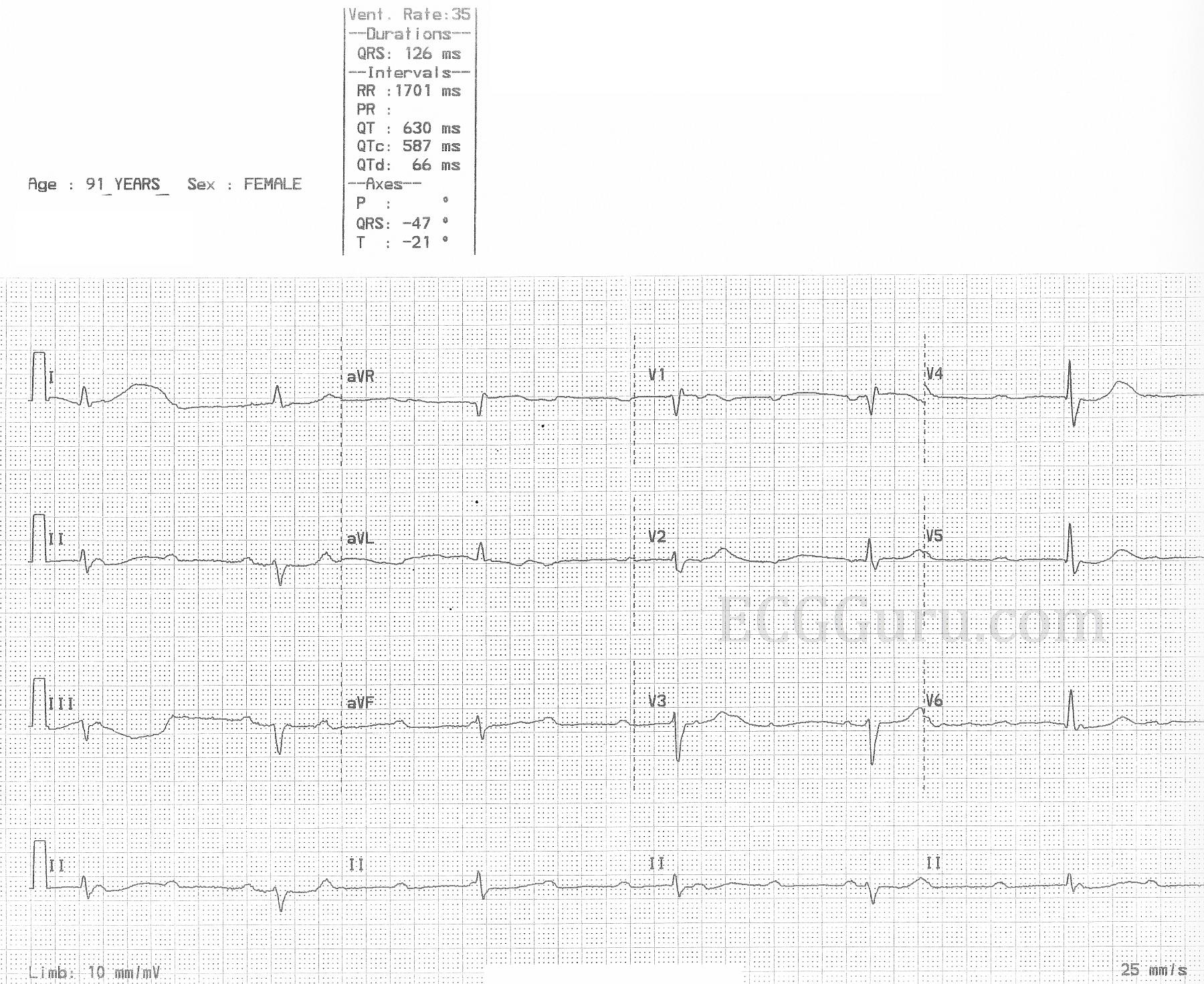
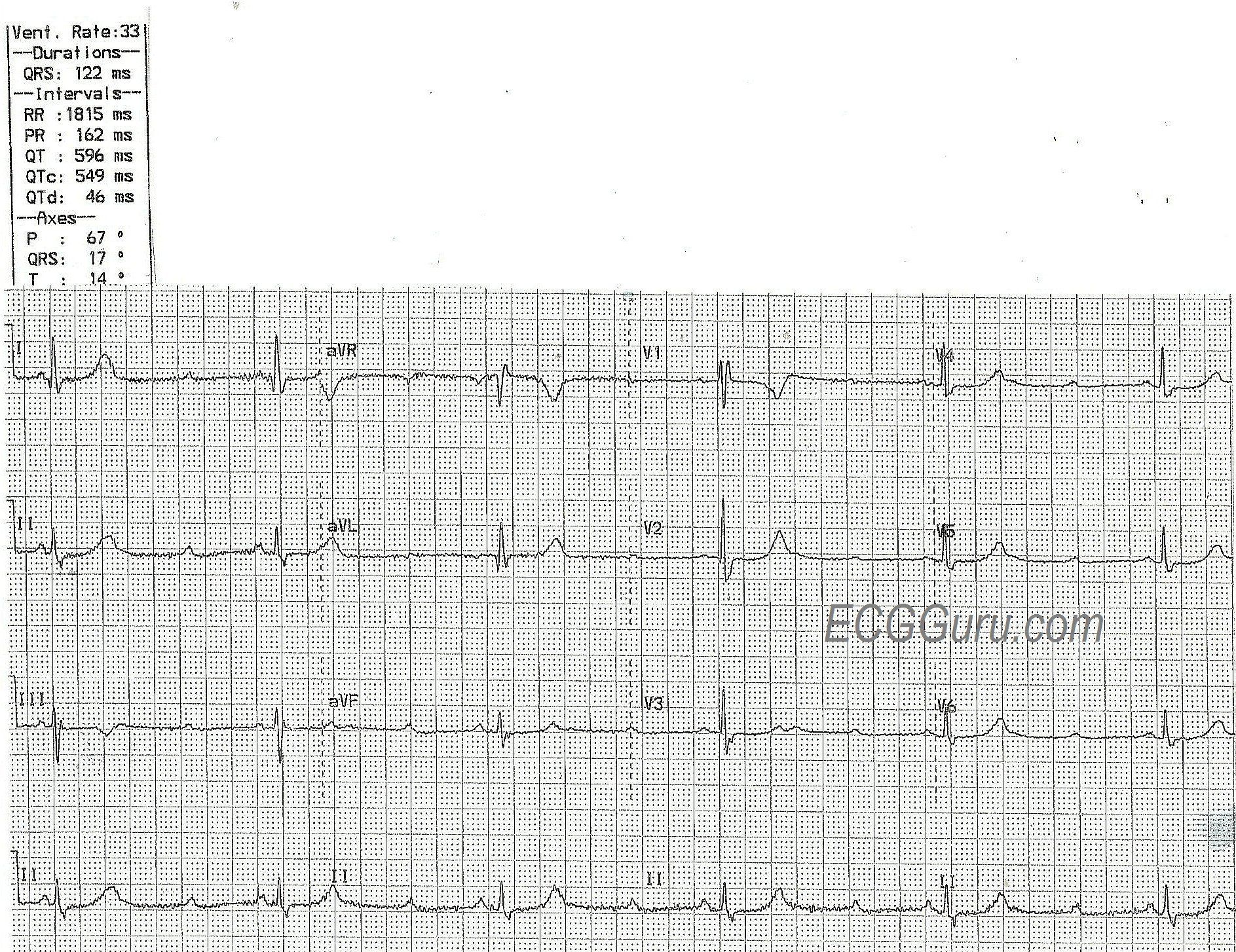
The patient in this example was having an inferior wall M.I. The ST elevation will not always show up on a monitor strip, as it does here. A 12-lead ECG is the minimum standard for evaluating for coronary artery disease and acute M.I. It is possible that the 2:1 block will disappear when the atrial rate (about 108 here) is slowed.