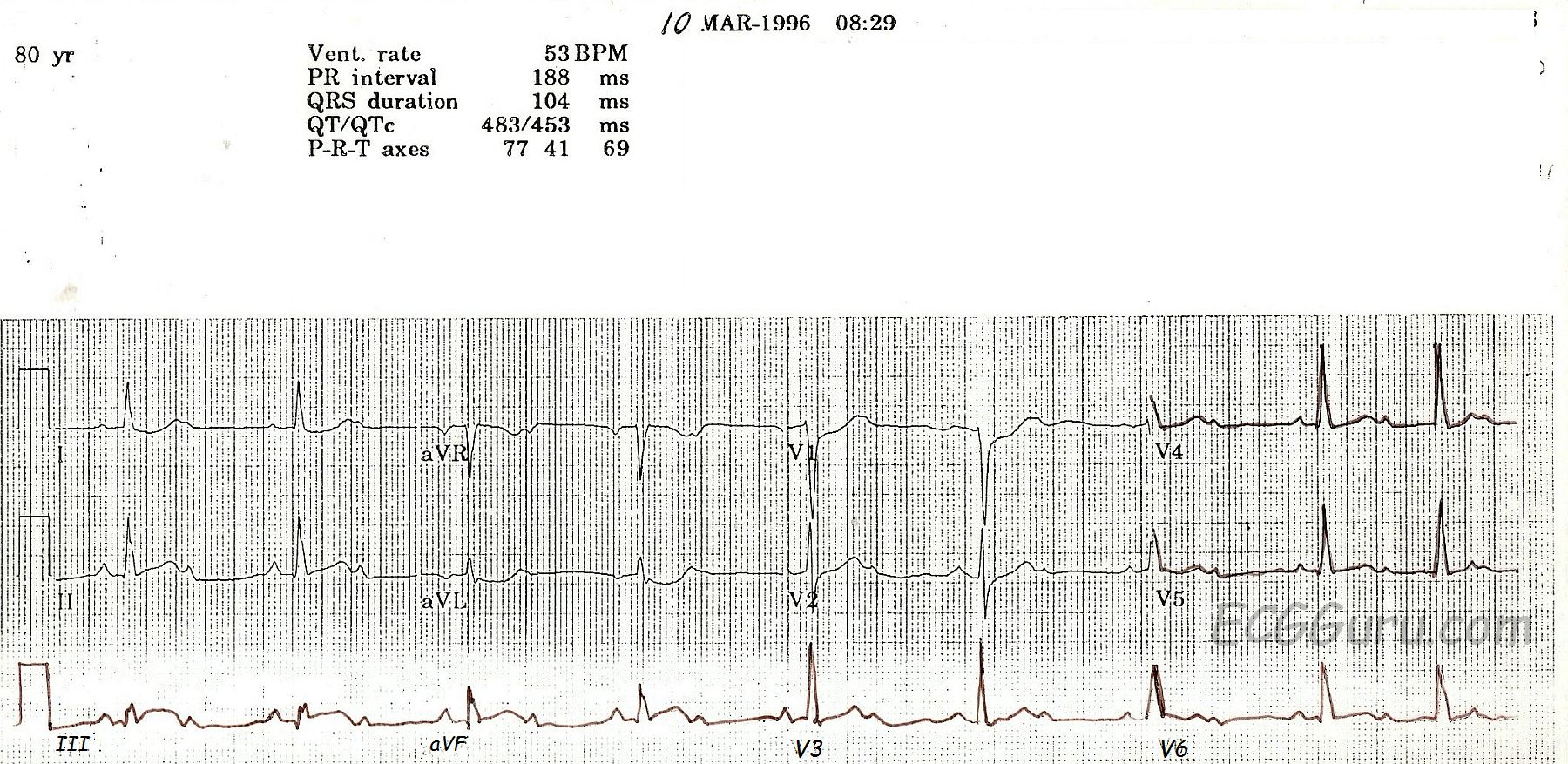
This ECG is from an 80-year-old woman who had an acute inferior wall M.I. with a second-degree AV block.
Some people incorrectly call ALL second-degree AV blocks that are conducting 2:1 "Type II". This is incorrect, as Mobitz Type I can also conduct with a 2:1 ratio. The progressive prolongation of the PR interval will not be seen with a 2:1 conduction ratio, because there are not two PR intervals in a row.
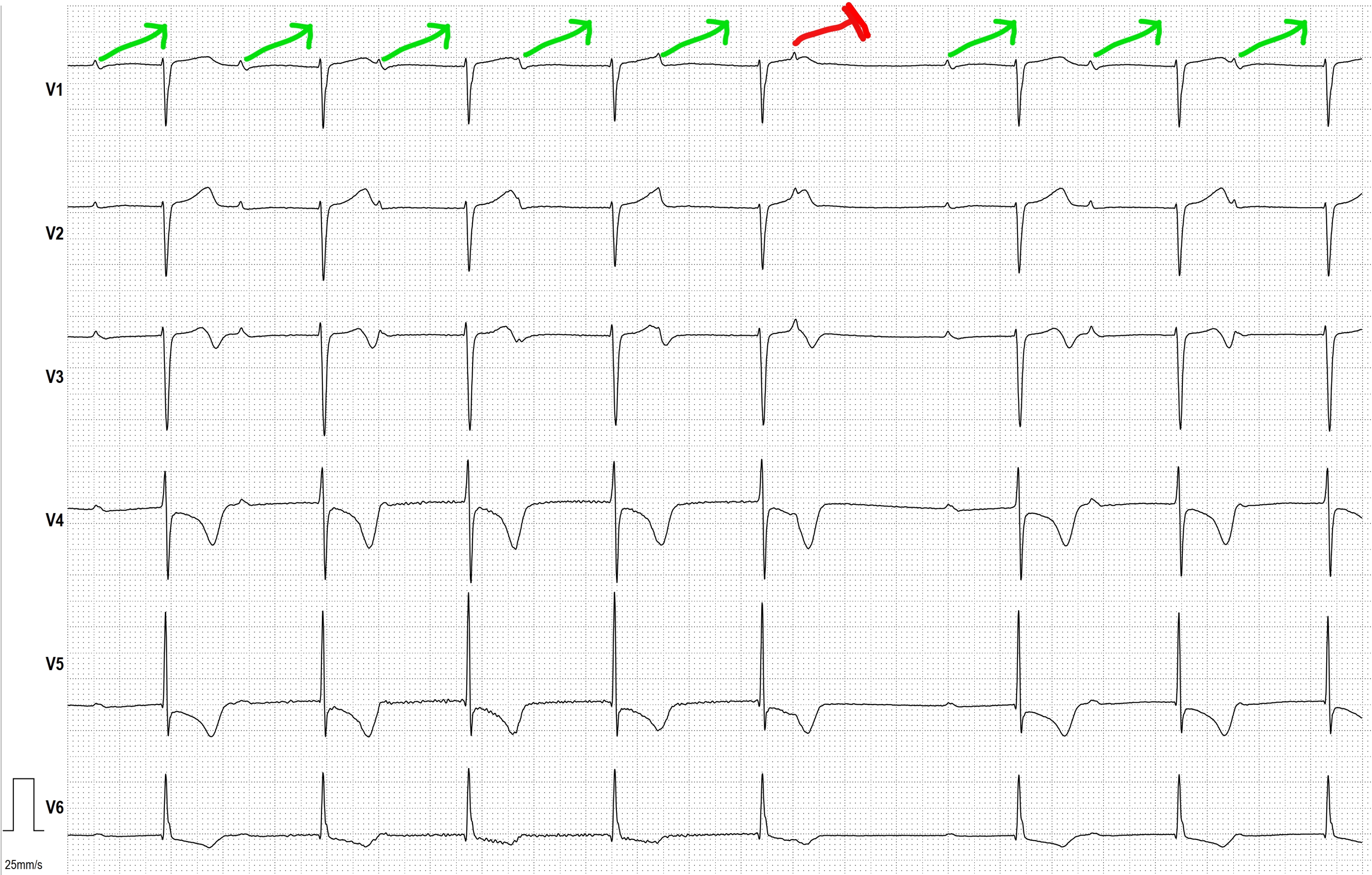
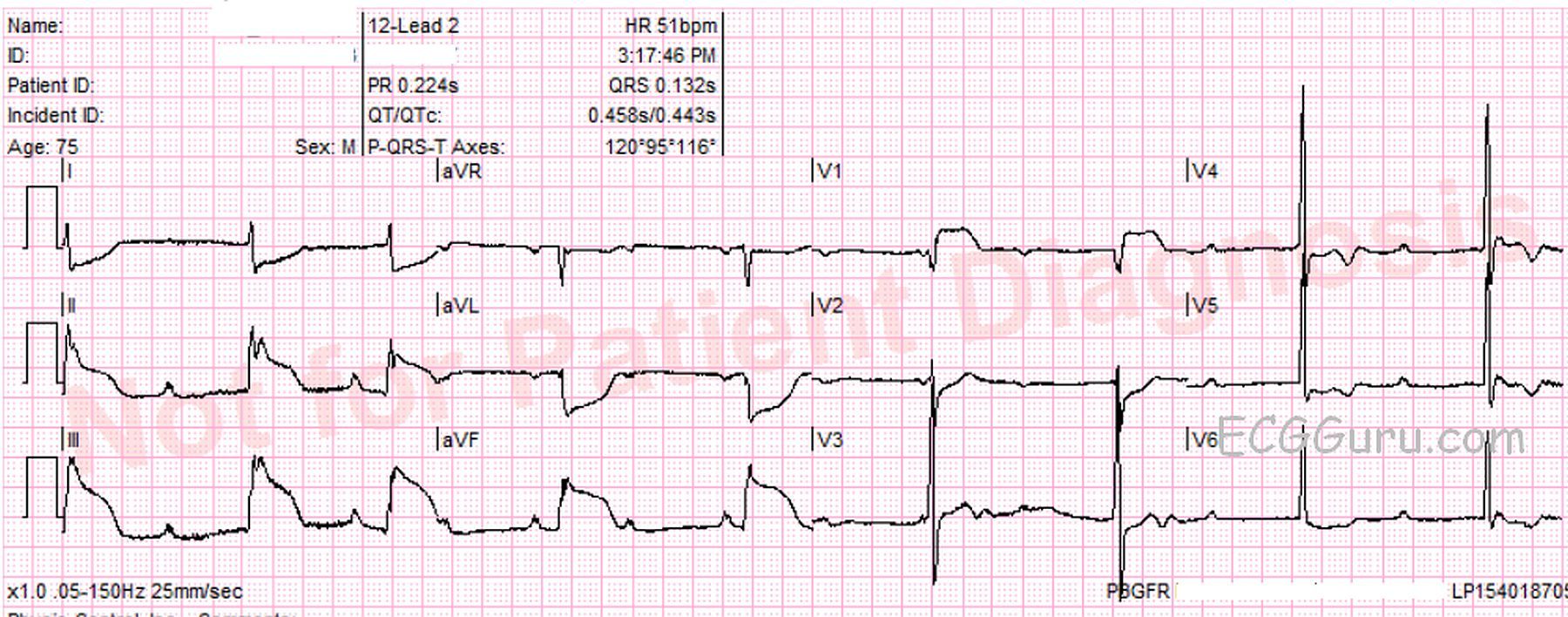
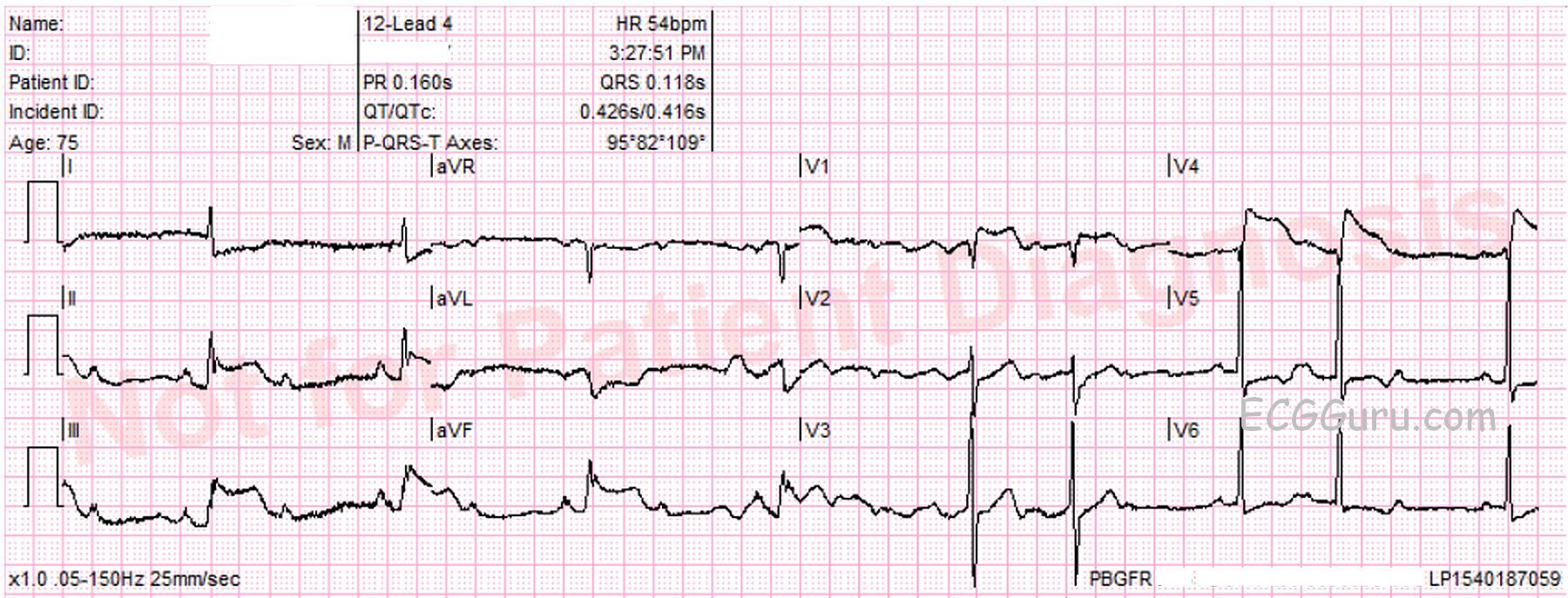
This is a good example of a Type I, or Wenckebach, block which is initially conducting 2:1. At the end of the ECG, two consecutive p waves conduct, showing the "progressively-prolonging PR interval" hallmark of a Type I block. Type I blocks are supraHisian - at the level of the AV node - and generally not life-threatening. Blocks that are conducting 2:1 present a danger, however, in the effect they have on the rate. Whatever the underlying rhythm is, the 2:1 block will cut the rate in half! This patient has an underlying sinus tachycardia at 106, so her block has caused a rate of 53. In light of her acute M.I., that rate is probably preferable to the sinus tach. This patient’s BP remained stable, and she did not require pacing.
The ST signs of acute M.I. are rather subtle here. Note the "coving upward" shape in Lead III, and the reciprocal depressions in I, aVL, V1, and V2. Type I blocks are common in inferior wall M.I., since the AV node and the inferior wall often share a blood supply - the right coronary artery.
While the print quality of this ECG is not the best, it is a great teaching ECG because it starts out with 2:1 conduction, then at the end of the strip, proves itself to be a Wenckebach block.