
Submitted by Dawn on Wed, 08/07/2013 - 11:41
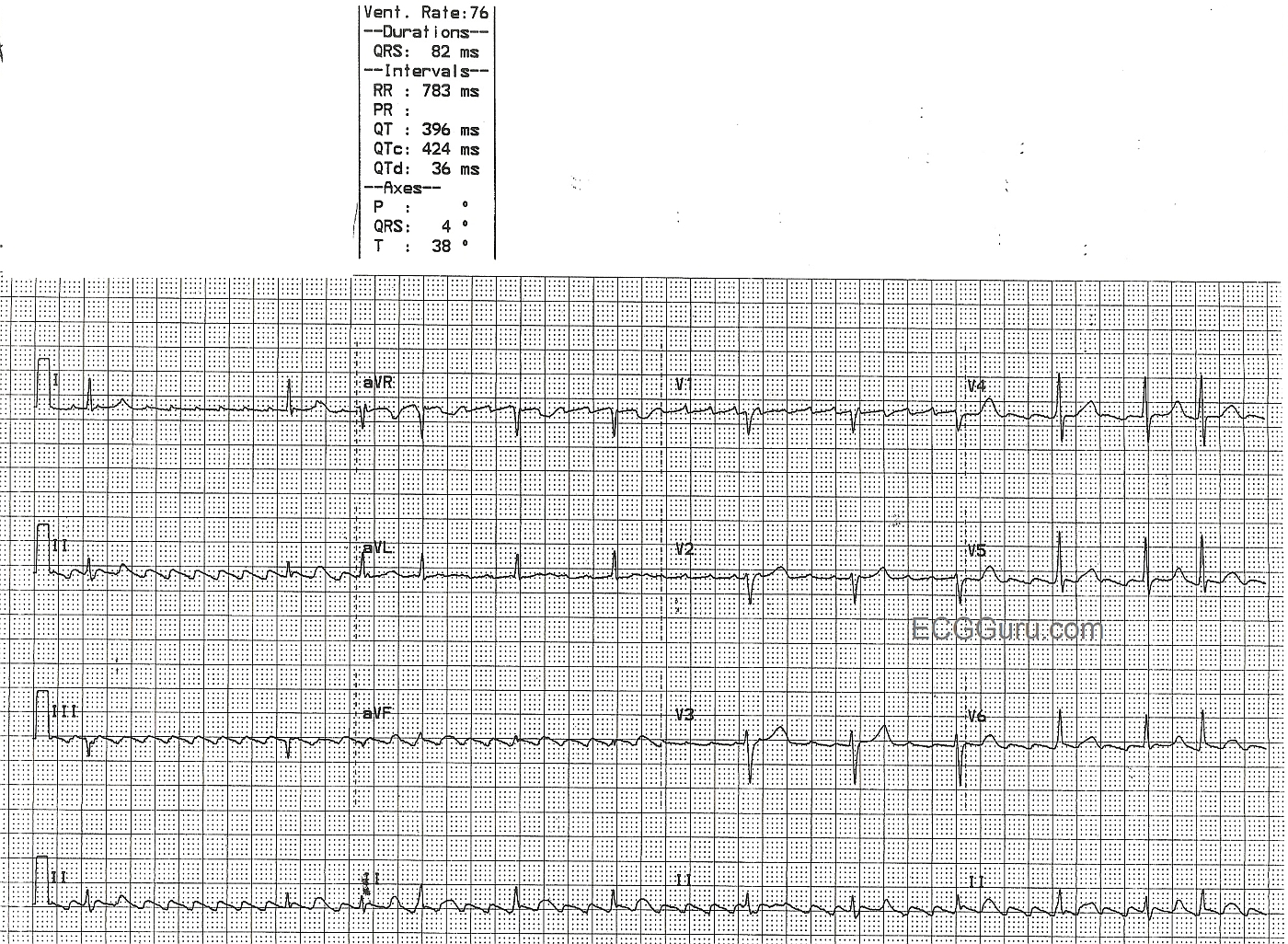
This ECG, showing atrial flutter with variable conduction, has good teaching points for all levels of students. The atrial rate is between 250 and 350 bpm, actually very close to 300 bpm, which is typical of atrial flutter. The flutter waves create a "sawtooth" pattern in most leads, but not all. One good teaching point, always evaluate an ECG in as many leads as possible and practical, since the signs you are looking for may not be very obvious in all leads. In this case, V4, V5, and V6 have subtle flutter waves, and a faster ventricular rate, making the "sawtooth" pattern difficult to discern.
The rhythm appears irregularly-irregular, mimicing atrial fibrillation. But, on closer inspection, one can usually find several distinct R-to-R intervals in atrial flutter with variable conduction. In this ECG, conduction ratios vary from 2:1 to 8:1, but the R-to-R intervals vary according to the ratio. Every time the ratio of P waves to QRS complexes is 4:1, for example, the R-to-R will be approximately .80 seconds (or a multiple of the P-to-P interval).
This ECG also teaches the beginner student to "march out" the P waves (flutter waves) THROUGH the QRS complexes and T waves, as the atria do not pause their fluttering while the ventricles depolarize and repolarize. The Lead II rhythm strip at the bottom illustrates this quite well.
For your more advanced students, this patient has low voltage, and we do not have patient information which would explain this in this particular case. The ventricular axis is close to 0 degrees, making aVF nearly isoelectric. You may have to magnify the strip for your students to find the QRS. Remind them that all four channels on this ECG were run simultaneously. So, if a QRS appears in aVR and aVL, it most certainly is present in aVF as well.
There are pathological Q waves in Lead III, but it is very difficult to evaluate for them in aVF, so their significance is unknown.
We eagerly await comments from our members. What do you think are the teaching points of this ECG - basic, intermediate, and advanced?
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Slow Atrial Flutter - Which Should Suggest some Diagnoses ...
As per Dawn - the rhythm of this 12-lead ECG is AFlutter (Atrial Flutter). The ventricular response is slow and variable. Although the R-R interval looks constant for a few beats toward the end of the tracing - the "F-R" (Flutter-QRS) interval preceding each QRS varies - so I do not believe there is any sustained fixed AV conduction ratio. It is important to remember that next to 2:1 and 4:1 AV conduction - that a variable ventricular response is the next most common AV conduction pattern seen with AFlutter.
As noted by Dawn - overall QRS voltage is reduced. This is a nonspecific finding. In addition there is a QS complex in lead III. That said - an isolated Q wave in lead III (even if large) may normally be seen, and is not necessarily indicative of prior infarction.
The most remarkable finding about this case of AFlutter is the slow ventricular rate - which is under 40/minute in the early part of the tracing. Unfortunately - we know nothing about the clinical situation - not even the age of the patient. That said - there is a differential diagnosis to consider whenever you encounter a patient with slow AFib or slow AFlutter:
IF the rate of AFib or AFlutter does not speed up after addressing these factors - then IF the patient is "older" - the diagnosis is probably SSS (Sick Sinus Syndrome) - and a pacemaker may be neededd if there are episodes of documented symptomatic bradycardia.
Ken Grauer, MD www.kg-ekgpress.com [email protected]