
Submitted by Dawn on Mon, 05/11/2015 - 01:15
Today’s ECG of the WEEK comes from Sebastian Garay, Paramedic. He presented it on his excellent website CardioCareConcepts.com, and was kind enough to share it with the ECG Guru. It is a great example of LEFT MAIN CORONARY ARTERY lesion with ST elevation in aVR and V1.
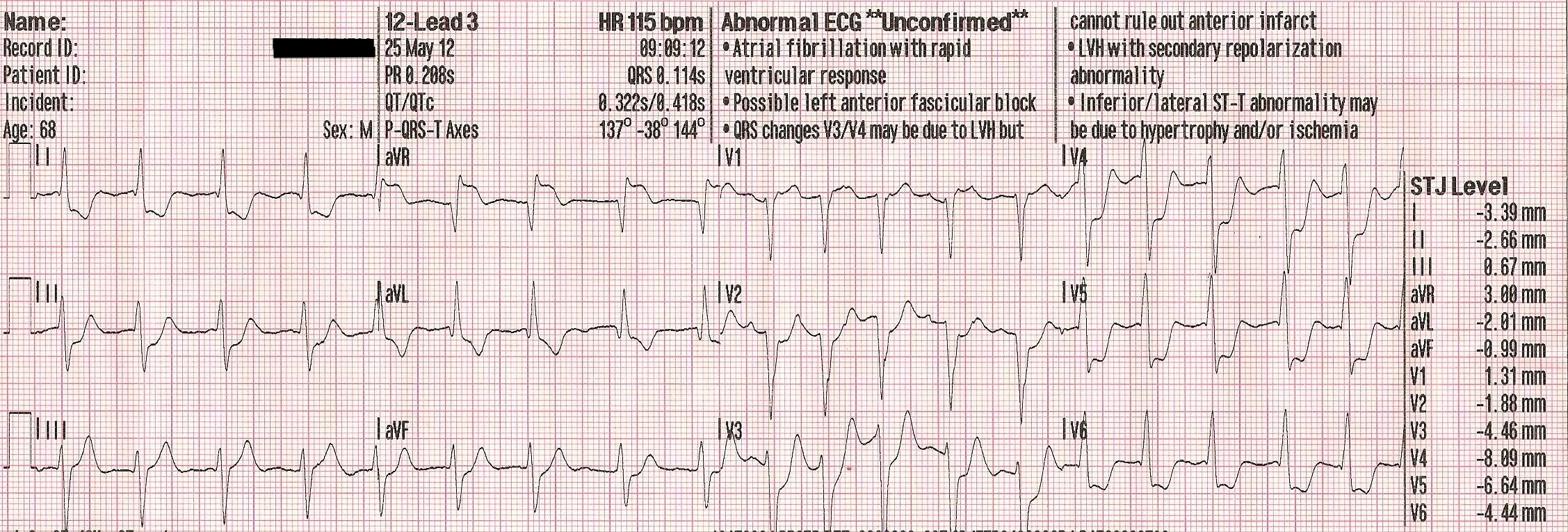
The patient was a 68 year old man who presented with a sudden onset of chest pain, followed by cardiac arrest. He was revived by the use of an automatic external defibrillator (AED). The initial 12-Lead ECG shows atrial fibrillation with a rapid response of 102 bpm. There are prominent ST ELEVATIONS in aVR and somewhat more subtle STEs in V1. These leads reflect the base of the septum, which is the area perfused by the proximal left coronary artery. A lesion in this area is sometimes in the LEFT MAIN coronary artery, or both the proximal LCA and the circumflex. Both of these types of lesions carry a very high mortality rate.
The widespread ST depressions reflect the injury current, which is being directed upward and toward the patient’s right shoulder, causing a reciprocal depression in all leads except aVR, V1 and Lead III.
This patient arrived in the Emergency Dept. in grave condition and was taken to the cath lab, where an occlusive lesion was found in the LEFT MAIN coronary artery. He later died from this severe injury.
We recommend further reading on this topic, as there has been a large body of research on ECG findings of ST elevation in aVR. Here are some links of interest:
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
ECG Distinction between LMain Disease vs Acute Occlusion
---------------------------------------------------------------------
Ken Grauer, MD www.kg-ekgpress.com [email protected]