
Submitted by Dawn on Sun, 06/24/2012 - 21:55
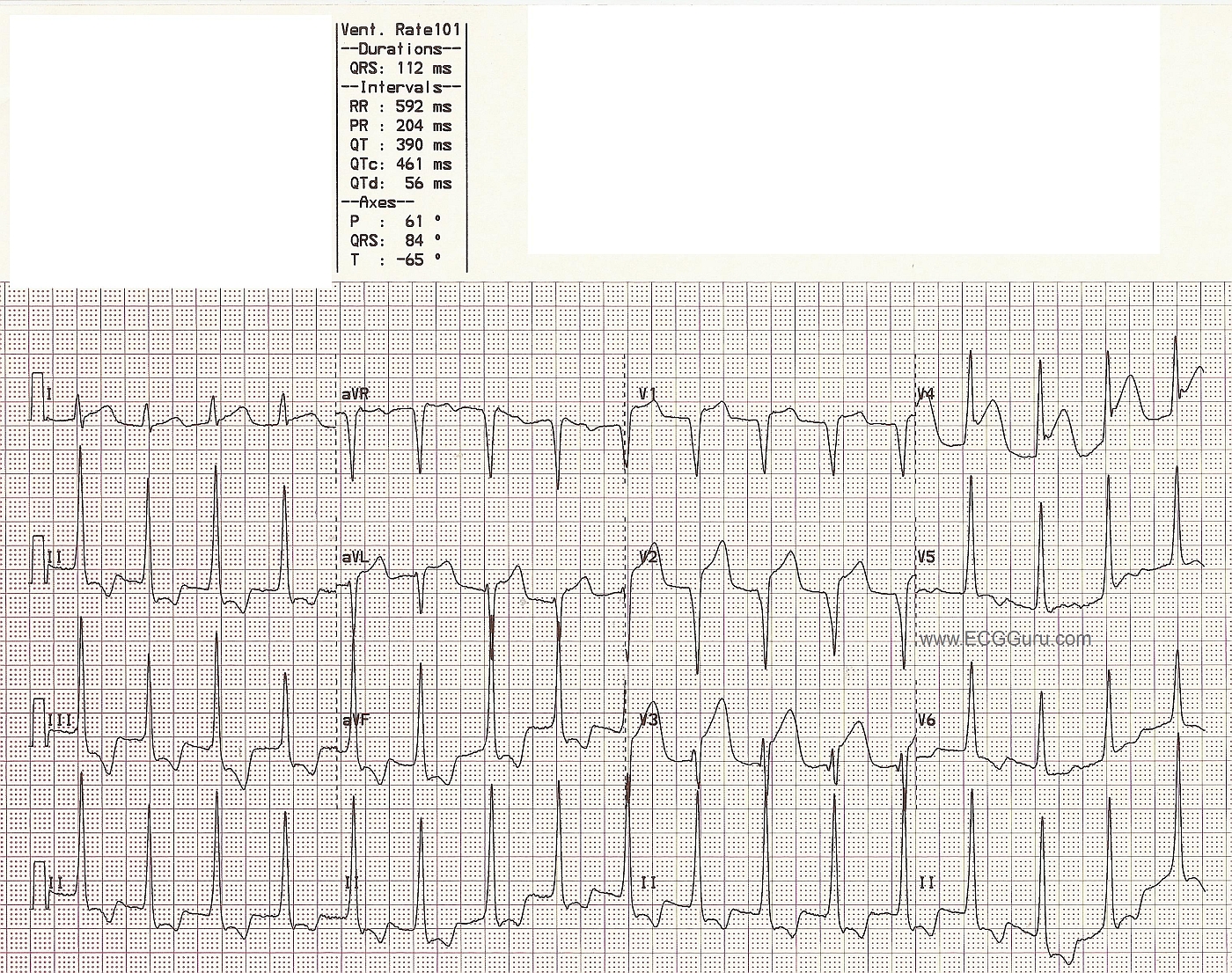
This is a good ECG for demonstrating the voltage and ST criteria for LVH and acute anterior wall M.I. in the same patient, where both conditions have been confirmed by other tests. If you are teaching the topics of ST elevation M.I., or left ventricular hypertrophy, you will probably have to address the issue that LVH can be considered a "mimic" for STEMI, especially for beginners. This is because LVH causes ST depression in leads with upright QRS complexes, and reciprocal ST elevation in leads with negative QRS complexes. This is called ST segment discordance. The ST changes in LVH are due to the "strain" pattern, indicating strain on the left ventricular myocardium. It is true that some ST elevation will appear in V1 and V2 in these patients, and can be mistaken for M.I. In the ECG shown here, the patient has definite ST elevation in leads which would NORMALLY have depression in the LVH strain pattern. Leads V1 through V4 have ST elevation that is not discordant, and is definitely real. This patient was taken to the cath lab, and his left anterior descending artery stented.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Some Additional Comments - re LVH and Ant MI at Same Time
Excellent point made by Dawn about co-presence of LVH and acute STEMI on this tracing. As stated - the distinction can at times be difficult. The bottom line to me is that you "need a human" to interpret the tracing. By that I mean that when there are "competing conditions" (ie, LVH and ant MI) - one can't put in a formula how to assess the relative contribution from each ...
Ken Grauer, MD www.kg-ekgpress.com [email protected]
P.S. One More Comment after a 2nd Look (7 months later!)
NOTE: I am writing this "P.S." Comment on January 26, 2013 - whereas I wrote my initial comment (shown above) on 6/28/2012.
--------------------------------------------------------------------------------
This tracing was just brought to my attention WITHOUT me realizing/remembering that I had previously seen and commented on it. That sequence of events itself is worthy of bringing up the well-known clinical reality of 10-20% expert intraobserver variation - when experienced electrocardiographers are subsequently asked to comment on a tracing they previously saw but without telling them what they said the 1st time! It is always interesting to me personally to see how "consistent" I am (or am not) in my interpretations of the same tracing at different points in time ... Regarding this ECG:
Ken Grauer, MD www.kg-ekgpress.com [email protected]