
Submitted by Dawn on Sat, 11/03/2012 - 00:06
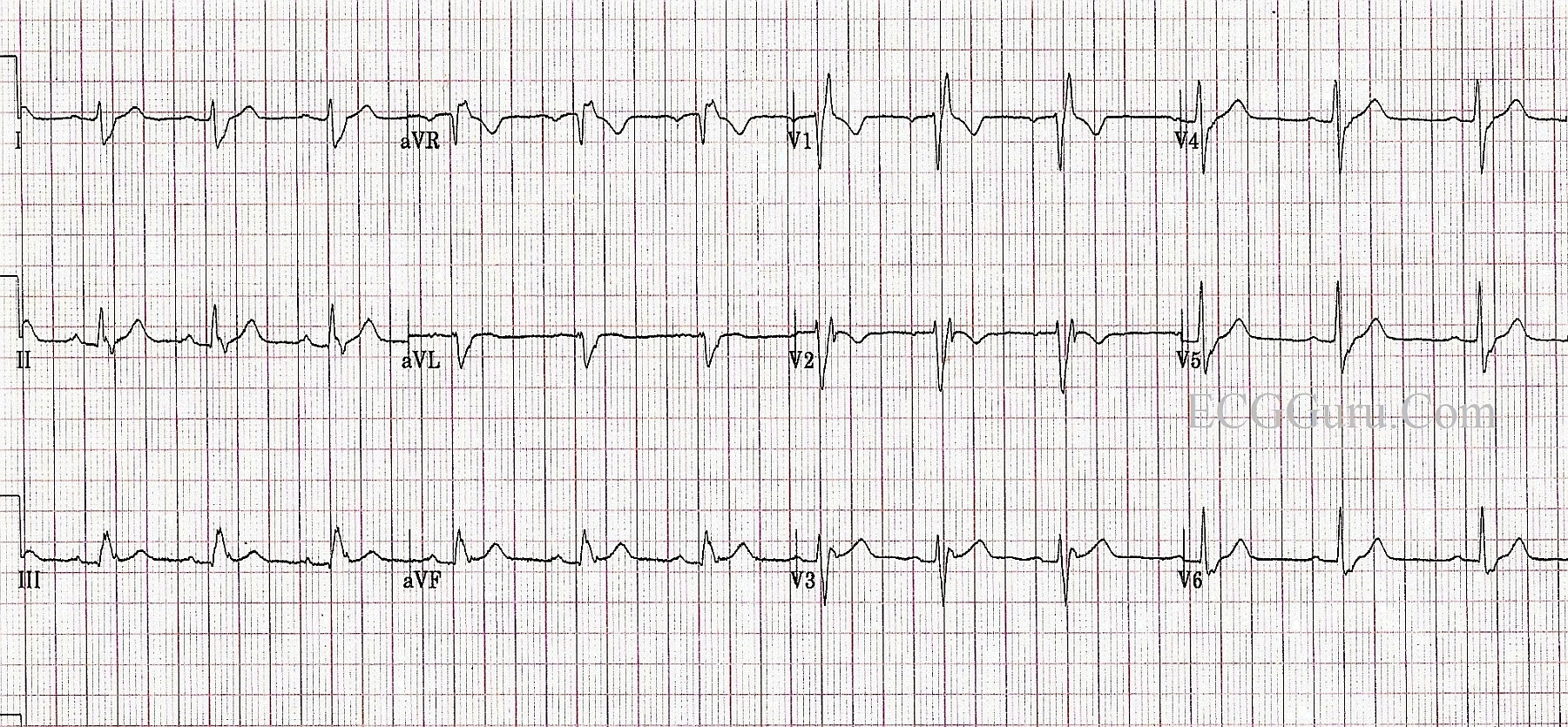
This ECG is from a healthy young man in his 20's. He was born with a ventricular septal defect (VSD) that was surgically repaired when he was a toddler. He now has a right bundle branch block, which could be a result of the defect, or the surgery. This is a good ECG for the Instructors' Collection because it clearly shows all the ECG characteristics of right bundle branch block: wide QRS in a supraventricular rhythm (in this case, NSR), rSR' pattern in V1, wide or "slurred" S waves in Leads I and V6. There is no rhythm strip below the 12 leads in this ECG, but there is no rhythm disturbance.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Nice RBBB - with 2 Additional Teaching Points
As per Dawn - the above ECG is a nice example of complete RBBB. There are 2 additional teaching points:
The 2nd teaching point I'd make - is that QRS morphology almost suggests LPHB (Left Posterior HemiBlock) in addition to RBBB. By far - LAHB (Left Anterior HemiBlock) is much more common than LPHB. This is because the left posterior hemifascicle is much thicker than the left anterior hemifascicle, as well as having a dual blood supply from both the right and left coronary arteries. The way to recognize this rare form of bifascicular block is to focus on lead I in a patient who has complete RBBB. IF R wave amplitude is small and the straight (unblocked) portion of the S wave in lead I is very steep - and, in addition you have predominantly positive QRS complexes in leads II, III - then the RBBB/LPHB form of bifascicular block is probably present. That's the case here.
For anyone interested - I've made a free download web page on the Basics of BBB at: https://www.kg-ekgpress.com/bundle_branch_block_pdf_file/
For a web page on the basics of axis and the hemiblocks - go to: https://www.kg-ekgpress.com/axis_basics-ecg/
Ken Grauer, MD www.kg-ekgpress.com [email protected]