
Submitted by Dawn on Sun, 02/03/2013 - 23:19
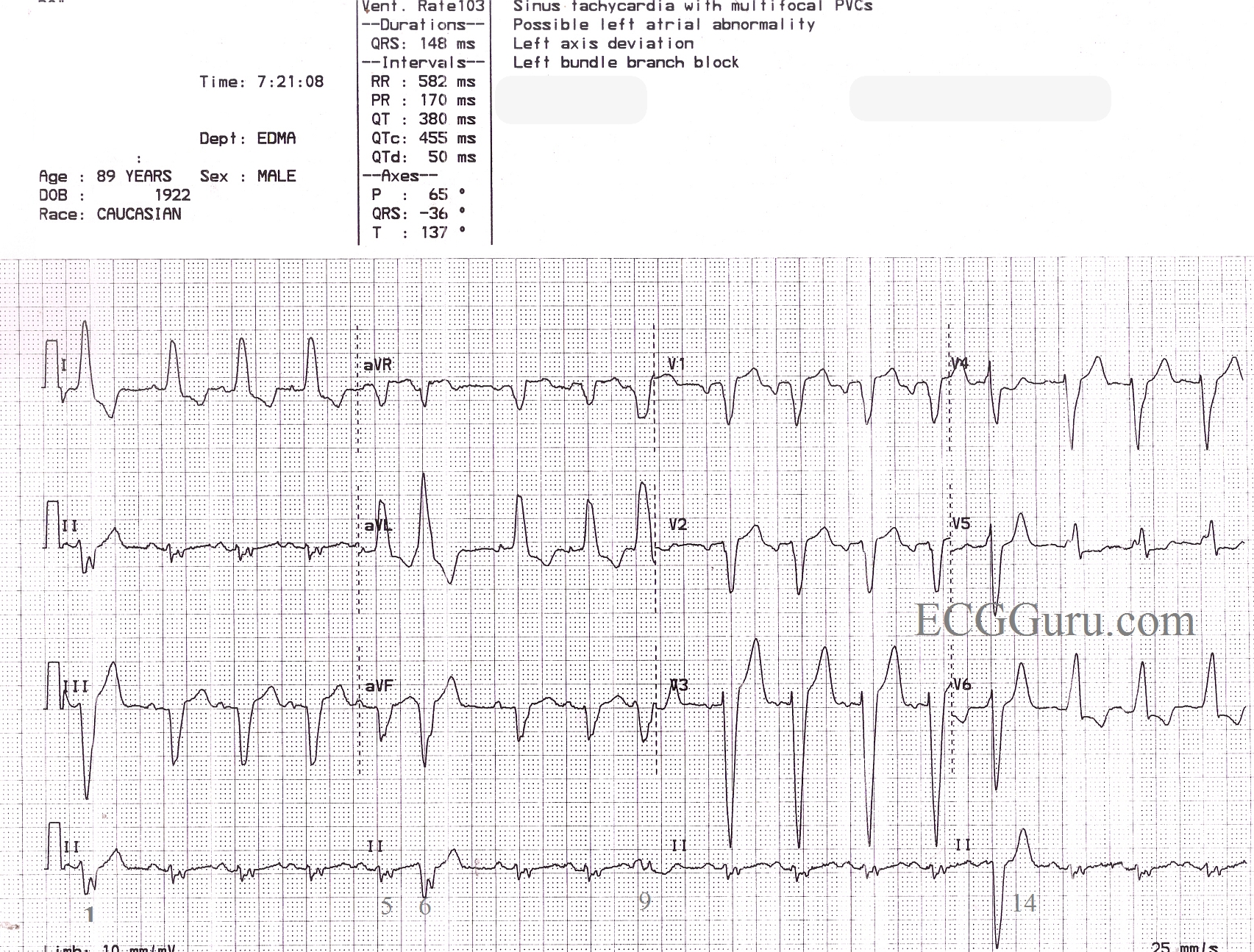
This is a great ECG for teaching your students about some of the different causes of wide QRS. This 89 year old man has a sinus rhythm that is around 100 bpm, and his QRS is widened at 148 ms (.148 sec). Leads I and V6 are positive, and Lead V1 is negative, meeting the criteria for left bundle branch block. There is a left axis deviation, which is common with LBBB, although it is not always this pronounced, indicating that there is possibly another cause for LAD. In this ECG, there are also PVCs and probable fusion beats. The 14th beat is a PVC. Complexes 1, 6, and 9 are possibly fusion beats. Fusion can be described as an almost simultaneous sinus beat and ventricular beat. The depolarization waves, one coming from the top of the heart and one coming from the bottom, meet and "fuse" on the ECG. Fusion beats will have some characteristics of the supraventricular beats and some of the ventricular beats. They are not significant except that fusion can be said to "prove" the existence of a ventricular pacemaker - either a natural pacemaker or an electronic one.
Do you see anything else interesting in this ECG? How would YOU describe this rhythm? Please do not hesitate to add your comments, or ask questions of the experts who contribute to this site. We will respond quickly to all questions.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
TITLE: LBBB and a LOT More Findings!
This is LBBB - plus a LOT more (the patient has had 89 years to get to this point - and it shows .... ). There are BASIC Teaching Points and many ADVANCED Teaching Points illustrated by this tracing which I'll comment on below.
The RHYTHM:
BOTTOM LINE re RHYTHM - It is not easy to be sure of what is going on. In situations like this - I find it best to state the generalities we can be sure of which is: Underlying sinus rhythm - multiform PVCs - possible PACs - there may be some fusion complexes.
-----------------------------
As to the REST of the ECG:
-----------------------------
OVERALL IMPRESSION:
-----------------------------
For anyone wth an interest - LINKS to:
Ken Grauer, MD www.kg-ekgpress.com [email protected]