
Submitted by jer5150 on Sat, 11/30/2013 - 10:34
The only patient data I have is that this ECG is from a 73-year old man. At the request of the site administrator (Dawn Altman), I'm posting this ECG because there isn't one quite like it in the Guru's archives. Some readers will recognize it as one I recently posted on another website. This one lives up to the title of "Challenging". I'll make the same general statement I did on the other website: You'll need to make careful measurements with calipers on this ECG to come to the correct interpretation.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
There are a few ways to see
There are a few ways to see this. one could argue bigeminal PAC's but it also looks like there are marching p waves and an irregular ventricular response which would raise a flag for mobitz I.
This is definitely a good strip!
J. Rudolph
http://jrudolph.com
Good and concisely interpretation!
Good interpretation, Dra Rudolph!
Good interpretation!
But I can see many more abnormalities.
Agree that the tracing is good. Do we expect more comments? It would be something fantastic.
Have a nice day.
1. Junctional rhythm
1. Junctional rhythm with right bundle branch block aberrancy at a heart rate of approximately 38 beats /minute. I think this is an independent rhythm-Junctional parasystole- with varying coupling intervals to sinus beats.
2. There is normal sinus rhythm after the 8th QRS complex at approximately 79 beats per minute.
3. There is AV dissociation between the aberrantly conducted junctional beats and sinus beats.
4. Aberrantly conducted beats do suggest old anteroseptal MI.
5. There is variation in the morphology of the p waves and rate to the left of QRS #8 for reasons I am not able to explain at this time but I thought I should start out with what I am able to contribute to the discussion for now.
Yes, I do agree that this is a highly challenging EKG and I look forward to more discussions on it and ultimately JASON’s interpretation. Thank you!
zafer karabulut
Good interpretation, Dra Rudolph!
Good interpretation, Dra Rudolph!
But I can see many more abnormalities.
Agree that the tracing is good.
INTERPRETATION
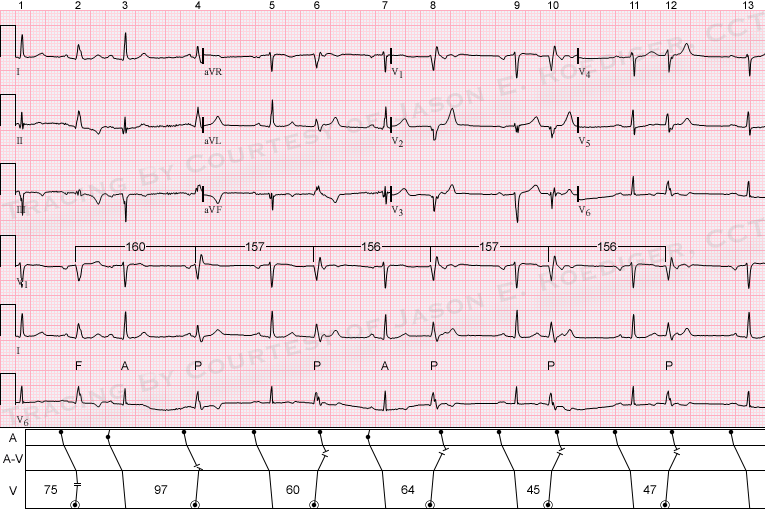
INTERPRETATION:(1.) Sinus rhythm (rate about 79/min) interrupted twice by . . .
(2.) . . . atrial premature beats (APBs; 3rd and 7th beats).
(3.) Ventricular parasystole (discharge rate about 37-38/min) producing a bigeminal pattern (see laddergram).
(4.) One ventricular fusion beat (2nd beat).
(5.) Old inferior infarction.
COMMENTS:
This patient had an inferior infarction 14 years earlier when he was 59-years old. The parasystolic beats (P) are dissociated from the sinus impulses rather than conducting retrogradely to the atria. While the "coupling" intervals vary widely between 45 and 97, the interectopic intervals remain relatively constant between 156 and 160. Parasystole is one of the more uncommon causes of a bigeminal pattern. At first glance, the atrial premature beats (A) are difficult to spot on the surface tracing but can be better seen on the laddergram. According to Dr. Marriott, some "play" of plus or minus 0.10s is allowed in the variation of the interectopic interval. Here they differ by only 0.04s. The discharge rate of ventricular parasystole has been reported to be between 38 and 60/min. Here it's at the lower-end of that range at 37-38/min. I think the ventricular fusion (F) is a good clue in favor of a ventricular origin rather than a junctional origin with aberration. Note in the laddergram’s ventricular tier that the parasystolic beats are represented by the dot within a circle.
Source/Reference:
(1.) Marriott HJL., and Conover, M.B.: Advanced Concepts in Arrhythmias. St. Louis: C.V. Mosby, 1998, p. 288-311.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]