Submitted by Dr A Röschl on Sat, 11/15/2025 - 05:40
When wide QRS complexes appear in an ECG, the question always arises as to whether they are supraventricular or ventricular in origin. The distinction may not be so important in the case of individual extrasystoles, but it is certainly important in the case of tachycardia. Ventricular tachycardia is always a serious finding, whereas SVT with aberrant conduction is initially considered harmless.
Submitted by Dr A Röschl on Thu, 04/24/2025 - 01:13
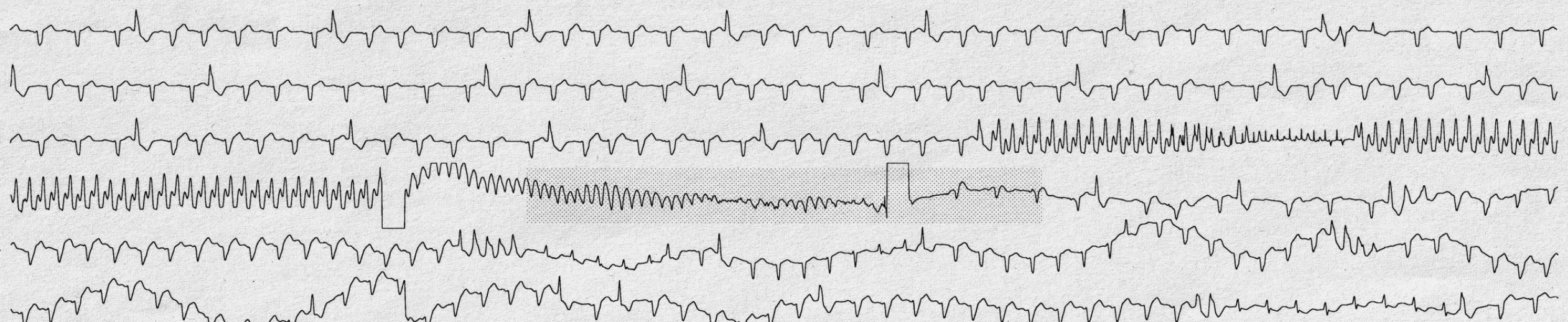
Sometimes a single Holter ECG can tell a whole story. Here we see a single-channel ECG, each line representing about 30 seconds.
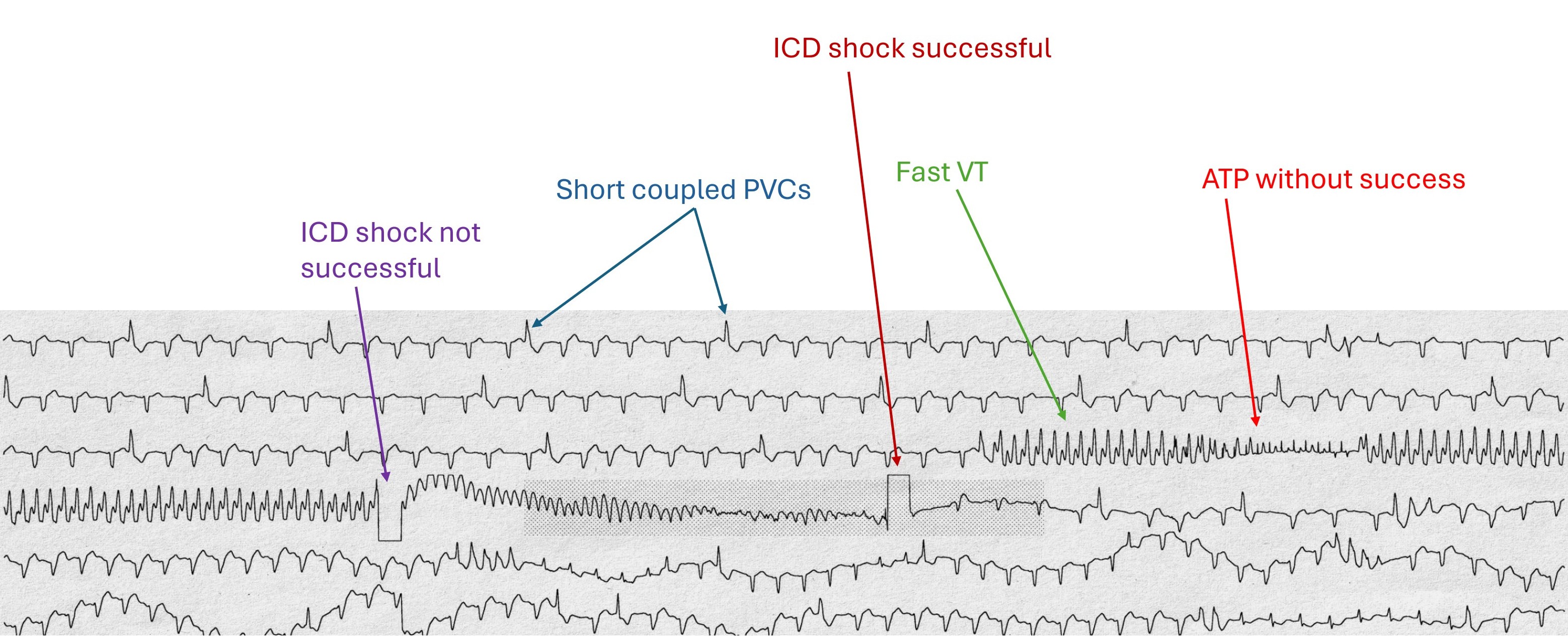
The ECG is from a 56-year-old man with severe ischemic cardiomyopathy who had an ICD implanted a few months ago due to recurrent ventricular tachycardia.
The explanation of what can be seen on this ECG can be found on the 2nd image.
Interestingly, the patient did not notice these events, they had occurred at night during sleep.
Submitted by Dr A Röschl on Thu, 04/24/2025 - 00:55
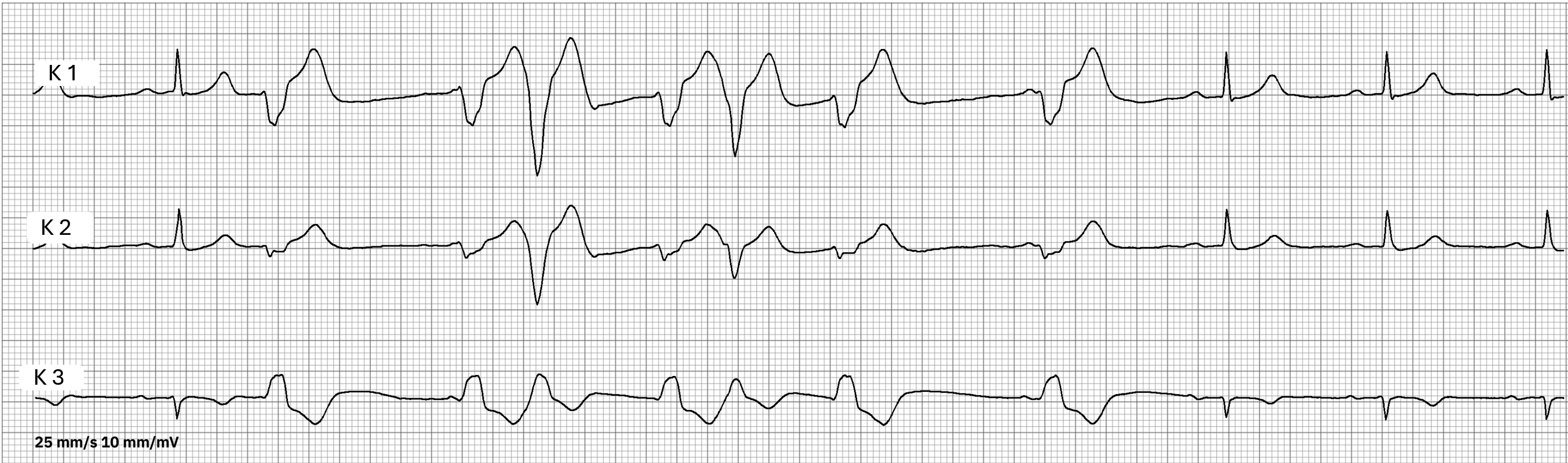
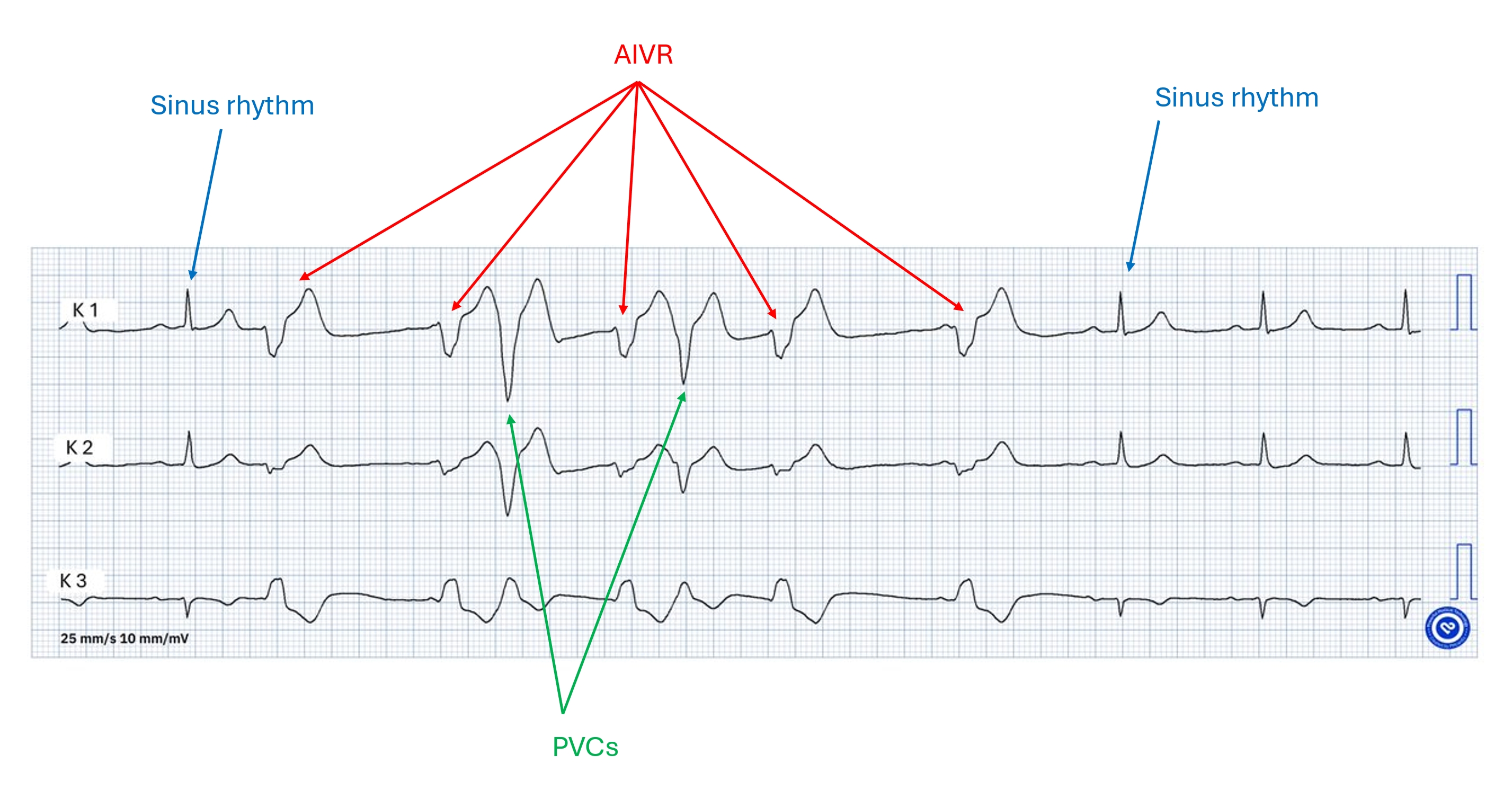
Here is a rhythm strip from a 3-lead Holter ECG. It comes from a 56-year-old man with arterial hypertension and no other previous cardiac diseases. Recently, the patient has noticed that pulse irregularities occur during blood pressure measurement (which he performs himself at home).
On the ECG, first a sinus beat, then a PVC, then an AIVR occurs, which is interrupted by another PVC, then sinus rhythm again.
Submitted by Dr A Röschl on Thu, 04/24/2025 - 00:29
Dawn recently posted an ECG with a 3rd degree AVB and an escape rhythm with narrow QRS complexes (junctional escape rhythm or escape rhythm from the area of the His bundle).
In addition, my ECG today is about a 78-year-old man with DCM who has noticed a significant increase in his existing shortness of breath over the last few days.
Submitted by Dr A Röschl on Mon, 02/10/2025 - 02:22
AV blocks are among the ECGs that are particularly difficult to diagnose and where the most mistakes are made.
Here is the ECG of a 75-year-old lady who has not been feeling well for the last few weeks and is complaining of shortness of breath on exertion.
The ECG is irregular with alternating smaller and larger RR intervals.
QRS 2, 4 and 6 each show the same PR interval; it can be assumed that these are sinus node beats that are conducted.
QRS 1, 3, 5, 7 are junctional escape beats without reference to the P waves.
Submitted by Dr A Röschl on Thu, 01/30/2025 - 03:40
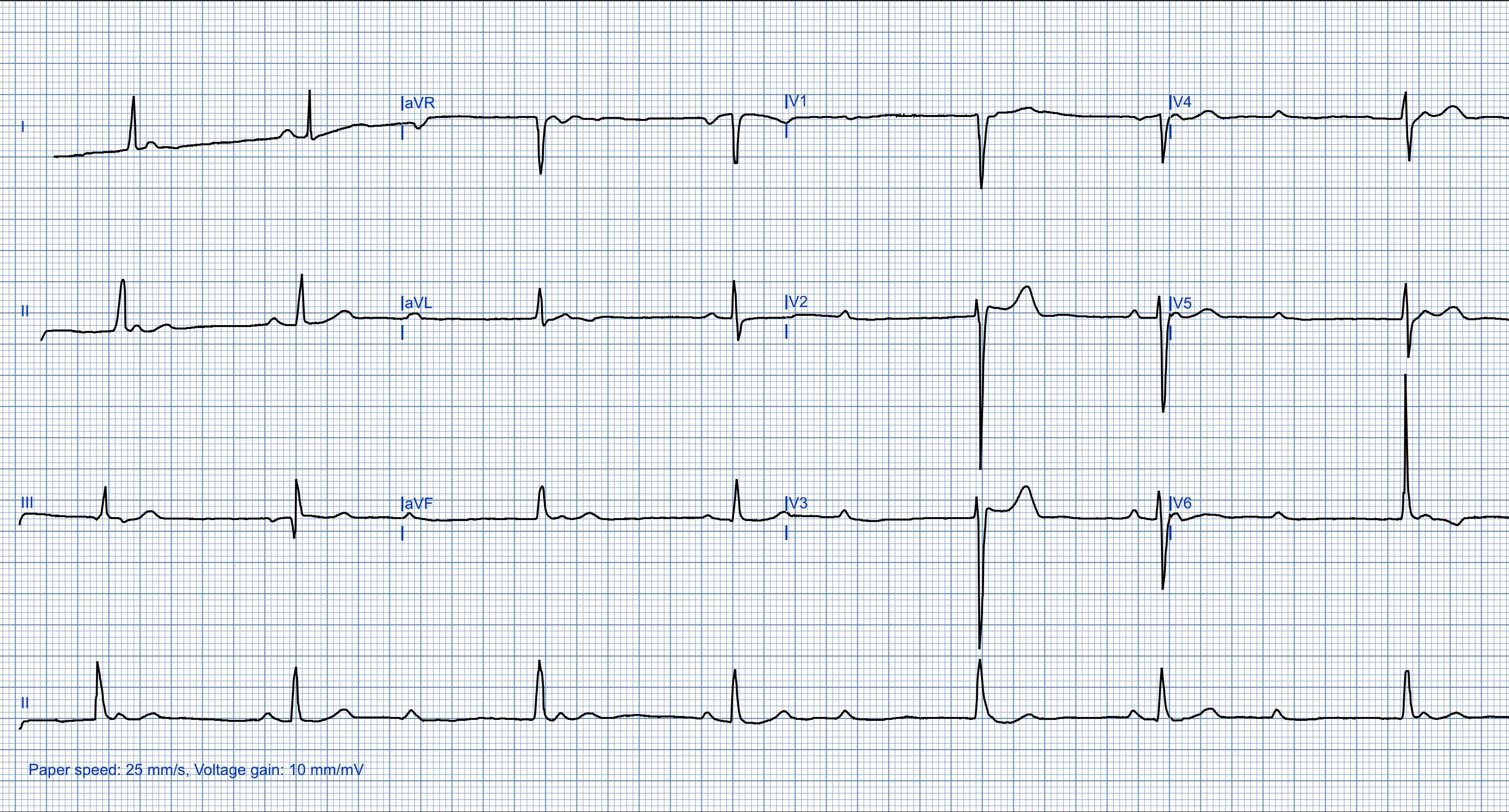
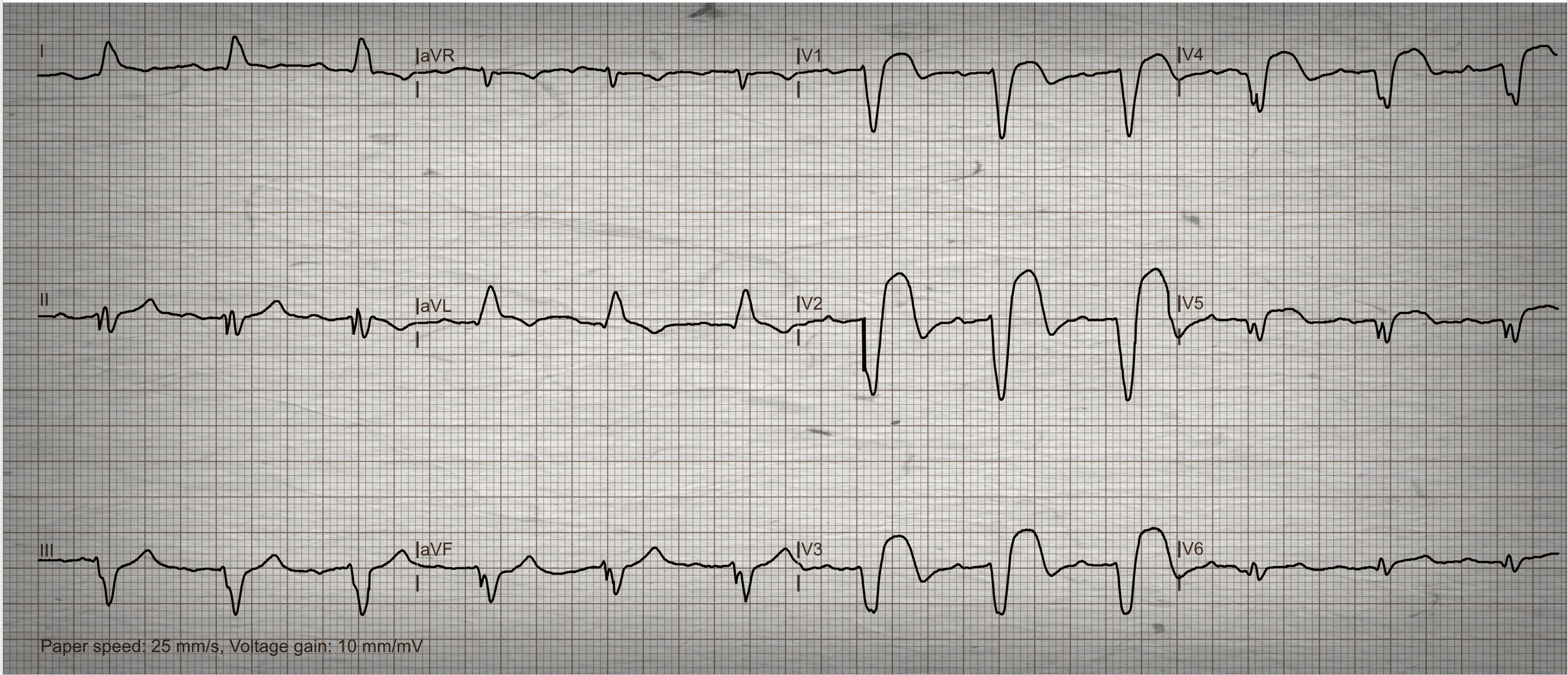
In this 12-lead ECG there is a bradycardic rhythm, which is regular, heart rate about 45 bpm. The QRS complexes are narrow.
What is this rhythm called?
There are no P waves present, and no flutter or fibrillation waves can be seen.
There are 2 possibilities:
1. There is a sinus arrest with a junctional escape rhythm. The junctional rhythm either cannot conduct retrograde to the atria (therefore no inverted retrograde P wave can be seen) or the retrograde P wave is hidden in the QRS complex (atria and ventricles are excited simultaneously).
Submitted by Dr A Röschl on Tue, 01/14/2025 - 02:03
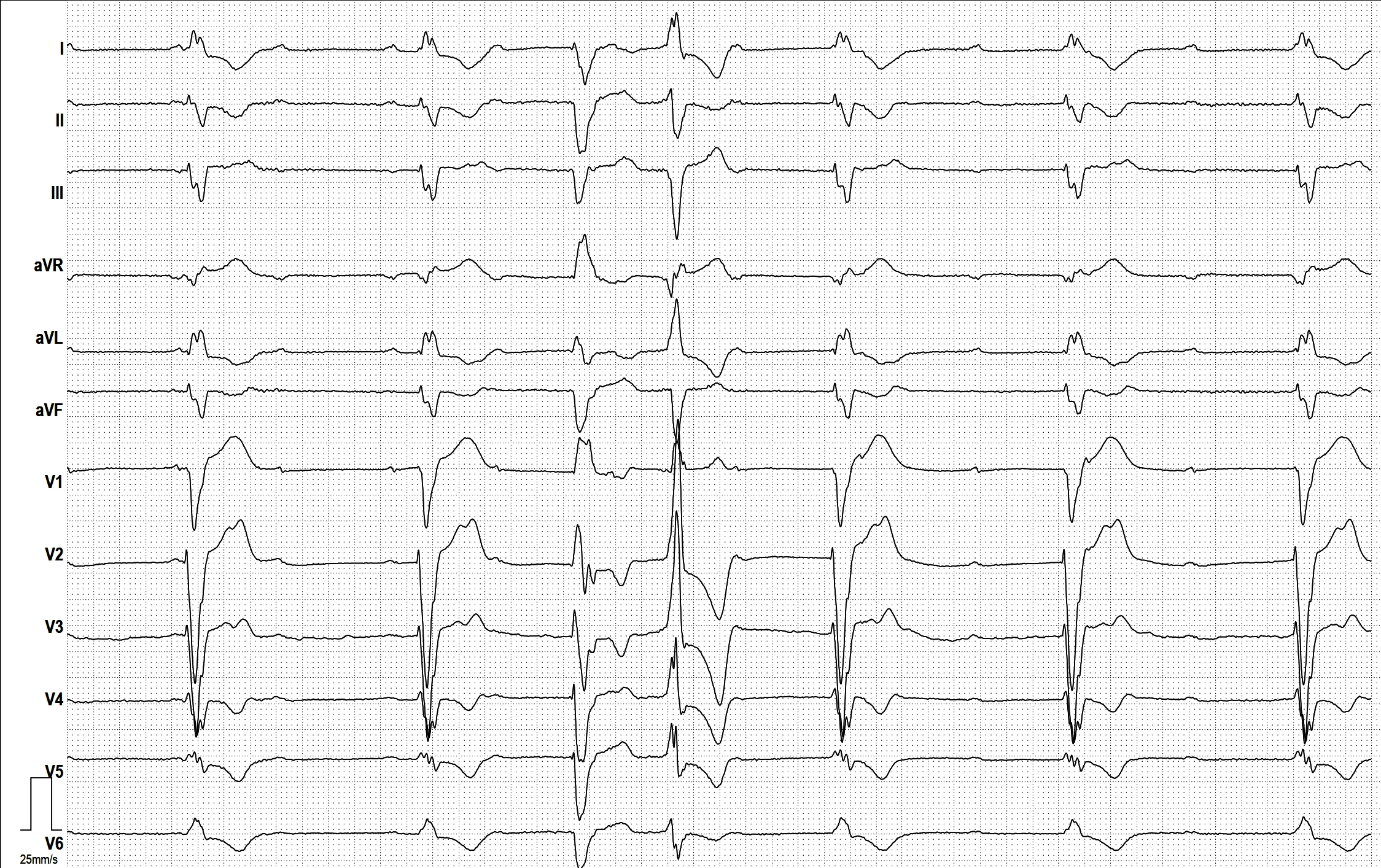
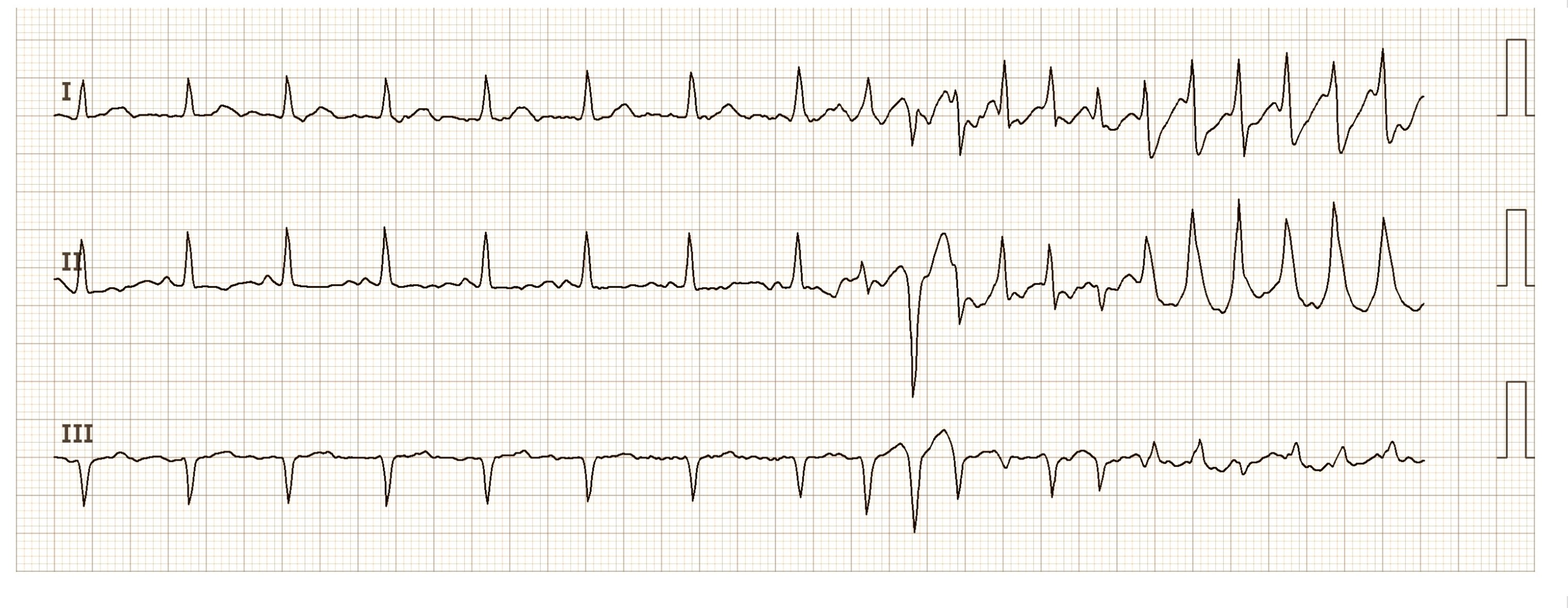
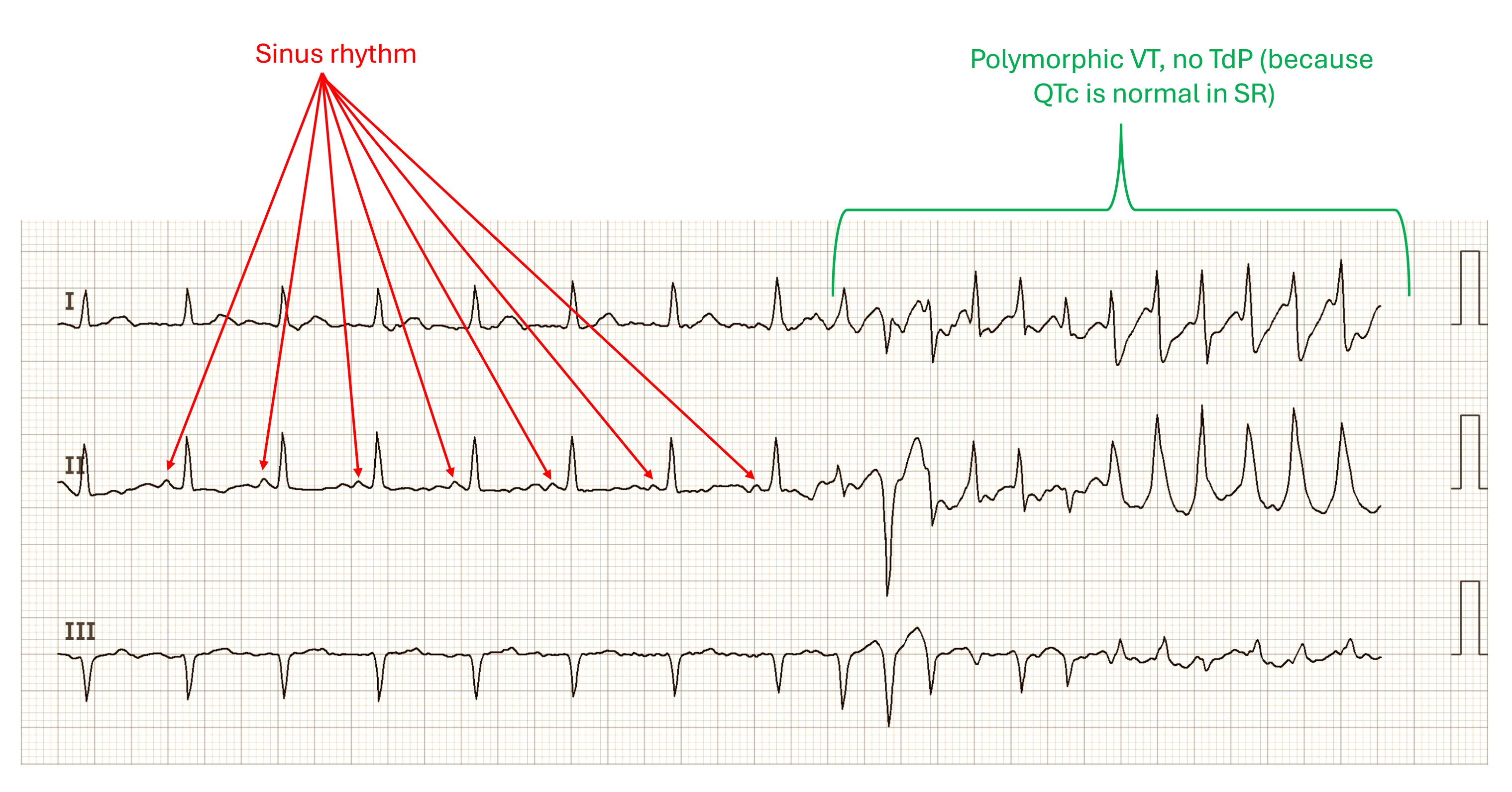
What can we learn from this 3-channel ECG?
A sinus rhythm can be seen in the left half of the image, which merges into a ventricular tachycardia on the right. The QRS complexes of the VT change their shape and polarity, this is called polymorphic.
The question is: can this be called TdP (Torsade de Pointes) tachycardia or not? The clear answer is: no! A polymorphic VT may only be called TdP if there is a prolonged QT/QTc duration in the native rhythm. This is obviously not the case here. Therefore, the term polymorphic VT is retained here
Submitted by Dr A Röschl on Tue, 01/14/2025 - 01:53
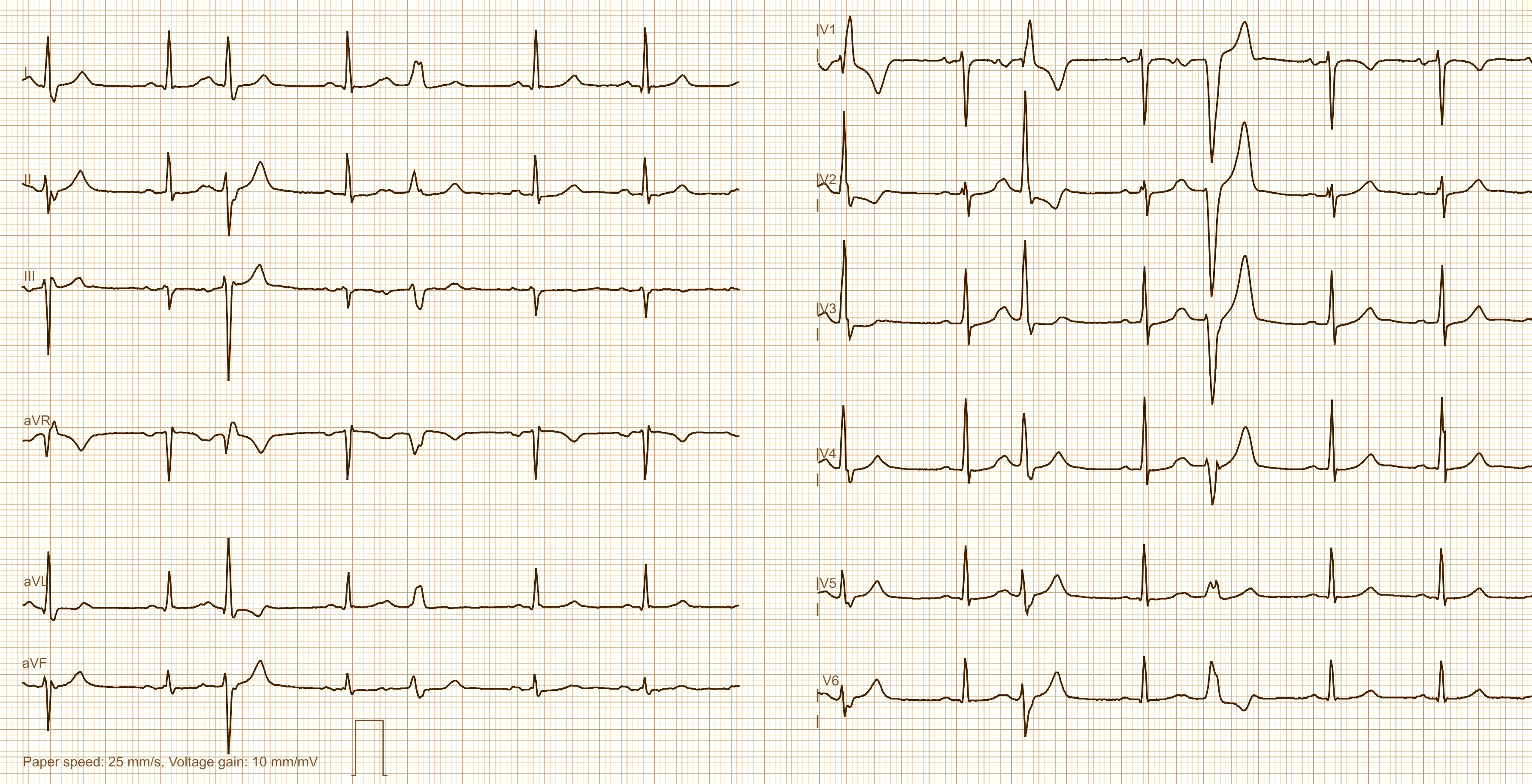
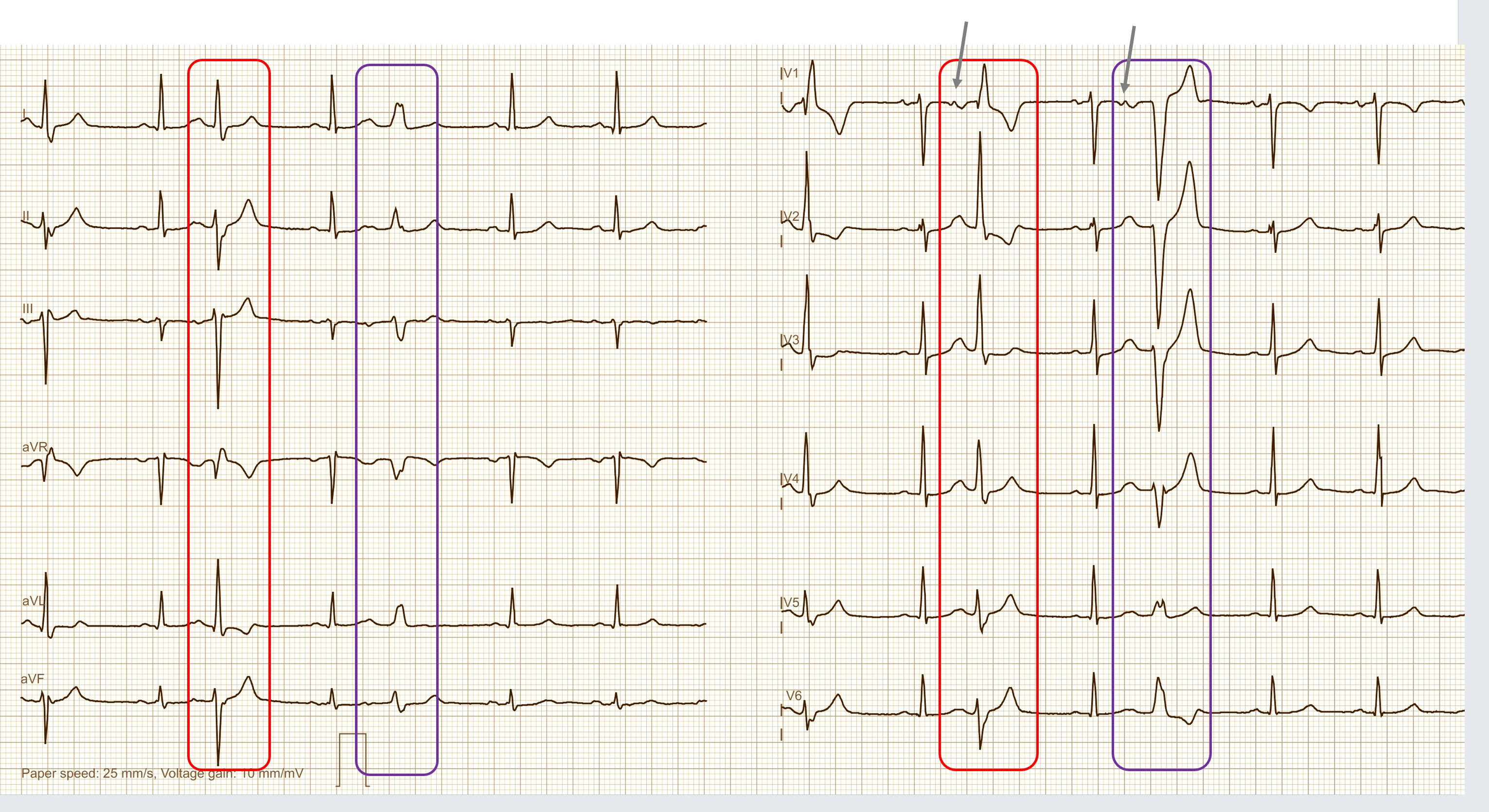
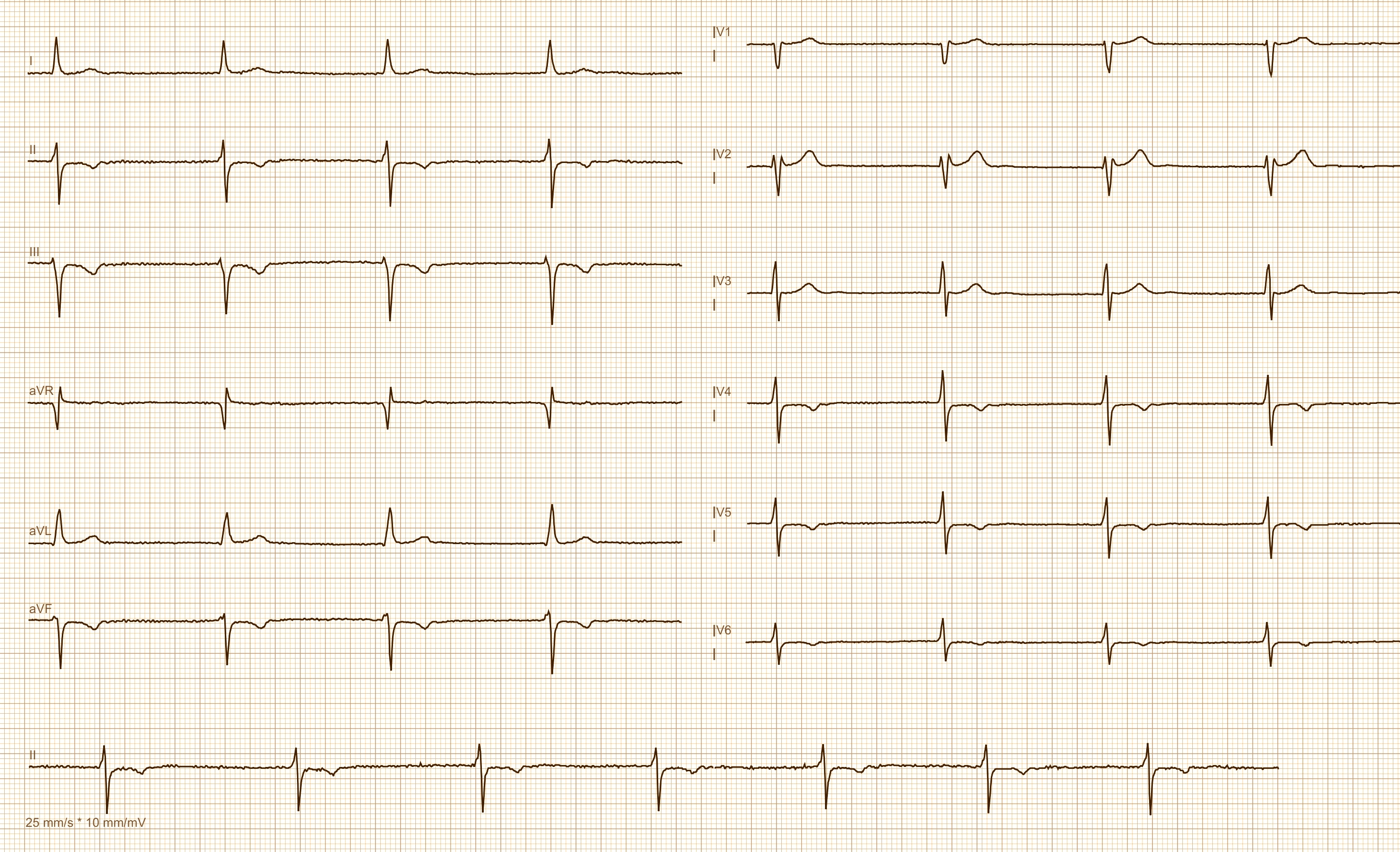
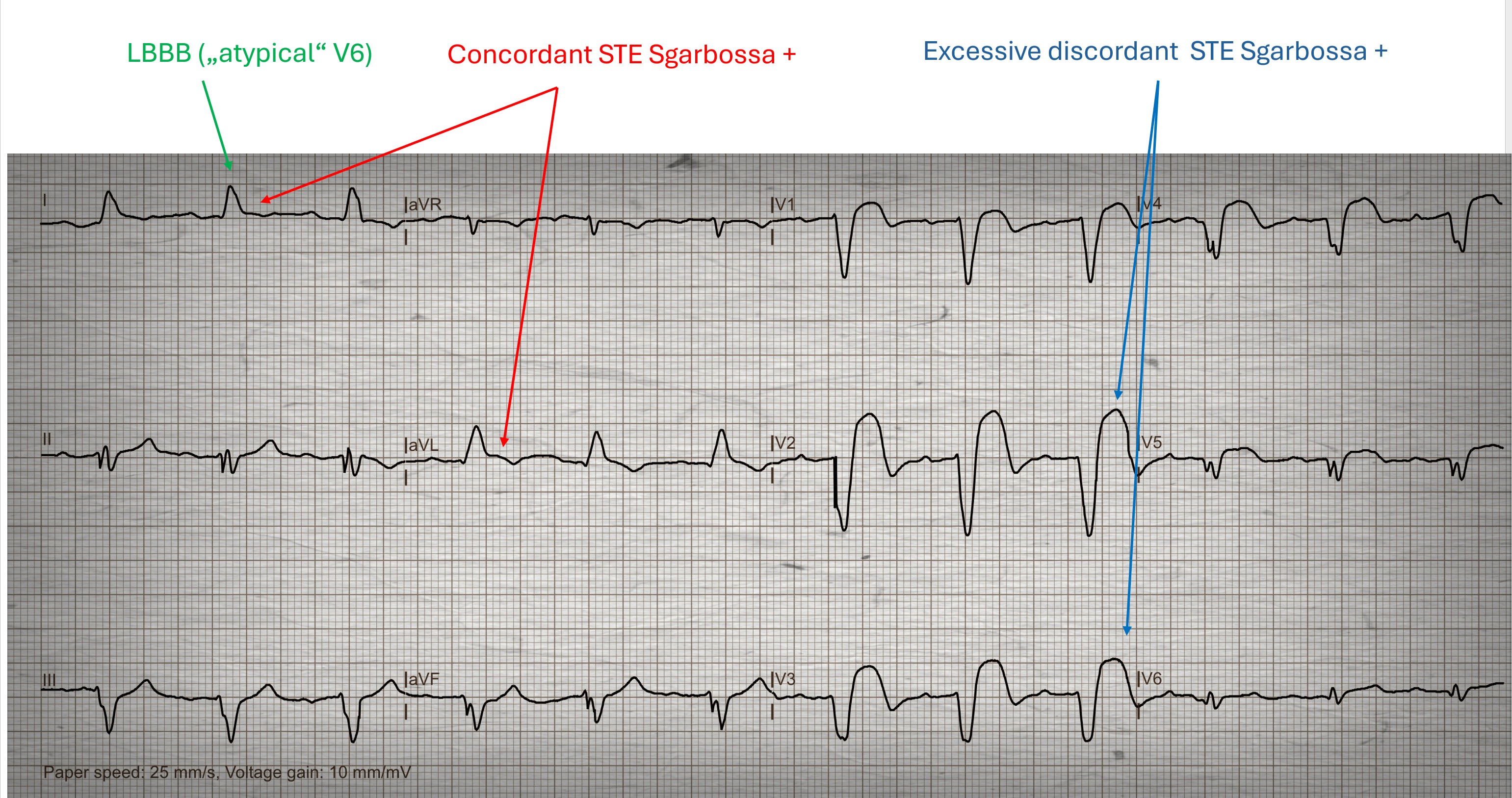
This ECG was sent to me by a friend, I don't know if he did it himself. The question was whether a heart attack can be recognized here. The patient is a 55-year-old man who has typical angina pectoris lasting more than 1 hour.
What can you answer?
Submitted by Dr A Röschl on Mon, 01/13/2025 - 01:49
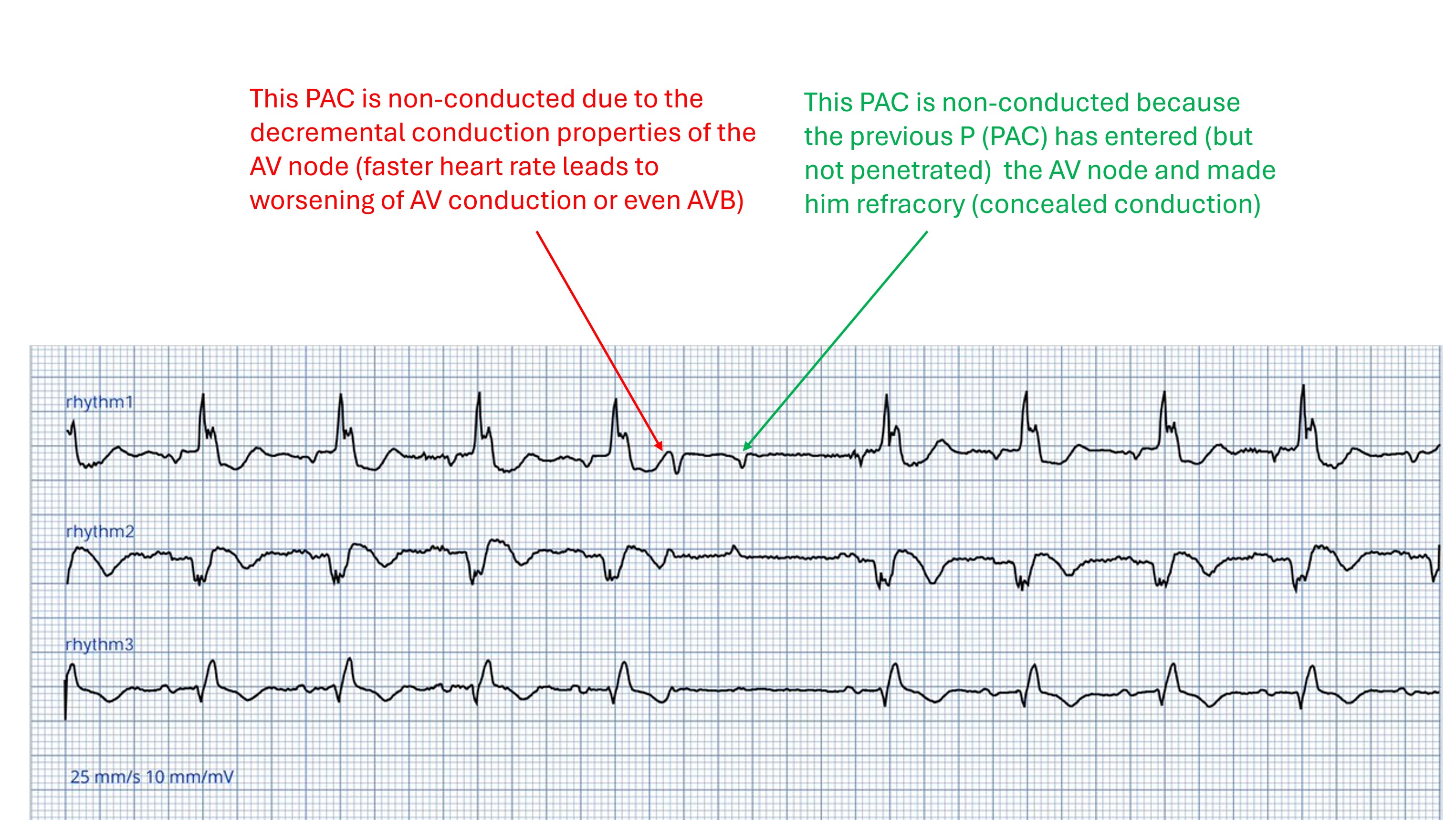
This ECG (3 rhythm strips) initially shows a sinus rhythm with 1st degree AVB grade I and wide QRS complexes (presumably RBBB pattern). A PAC (P-wave premature, different form than in sinus rhythm) appears approximately in the middle of the ECG, this is not conducted . Due to the strong prematurity, this is not surprising. But why is the 2nd PAC also blocked? The answer can be found in the second picture.
Submitted by Dr A Röschl on Wed, 01/08/2025 - 06:44
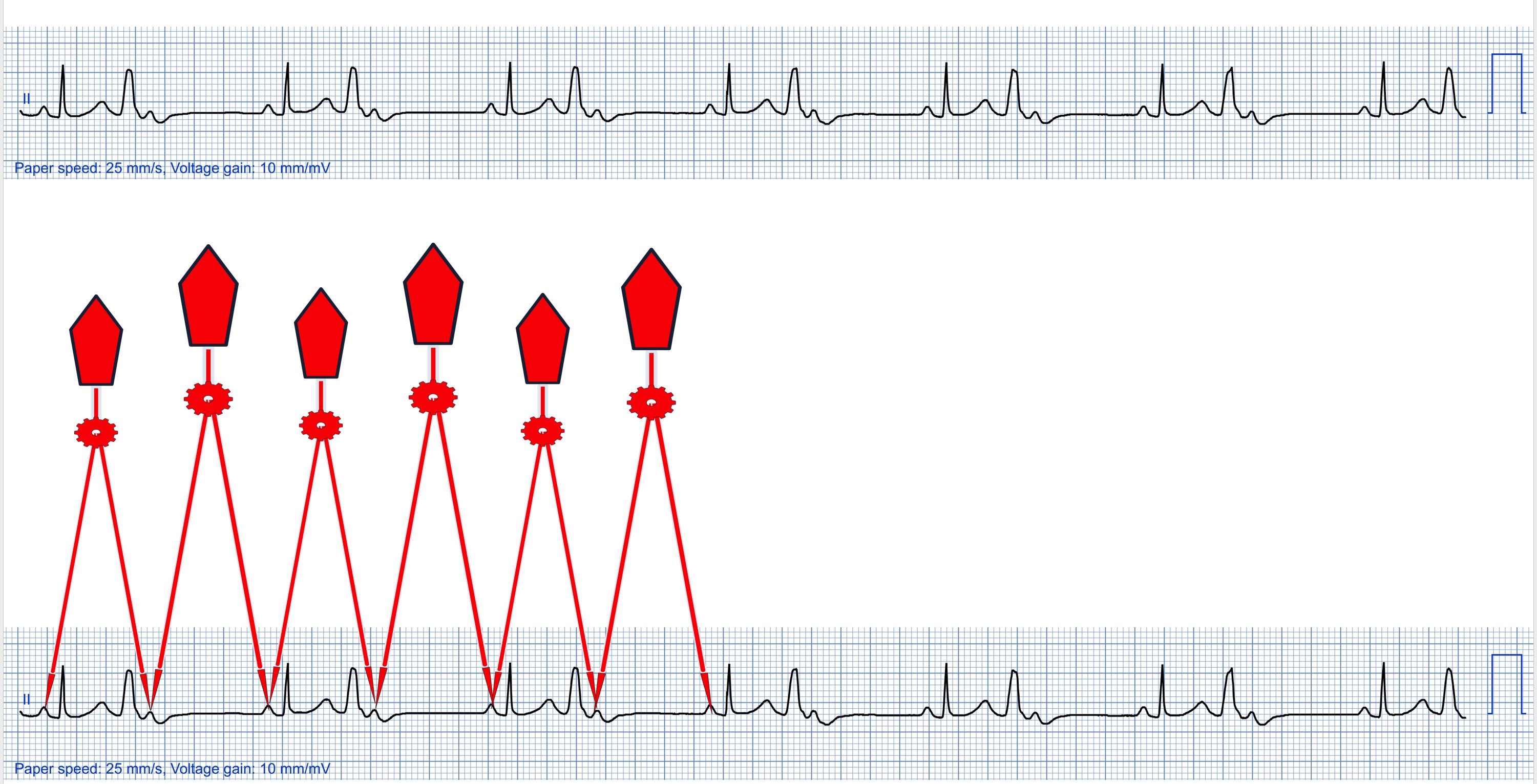
Sometimes in a simple 1-lead ECG strip, various interesting ECG phenomena can be recognized, such as here. One could briefly look over the ECG, make the diagnosis of ventricular bigemininy and then be satisfied.
On closer inspection, however, 3 questions arise:
1. Is the P wave behind the PVC a sinus node P or an atrial extrasystole?
2. + 3. after one comes to the conclusion that it is a sinus node P: why is it not conducted and why is the PP distance smaller when there is a QRS complex in between than when there is not.