
Submitted by Dr A Röschl on Wed, 01/08/2025 - 06:44
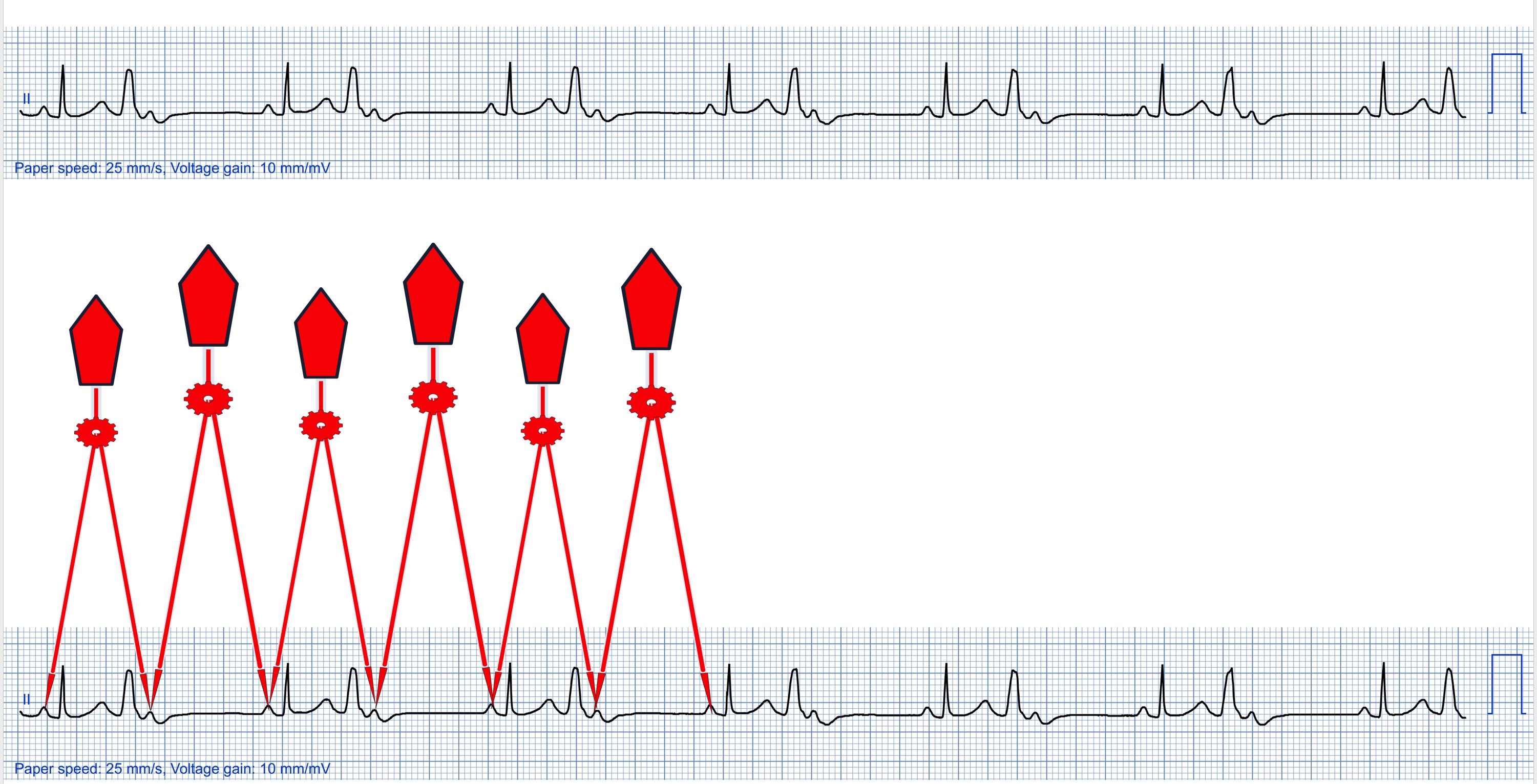
Sometimes in a simple 1-lead ECG strip, various interesting ECG phenomena can be recognized, such as here. One could briefly look over the ECG, make the diagnosis of ventricular bigemininy and then be satisfied.
On closer inspection, however, 3 questions arise:
1. Is the P wave behind the PVC a sinus node P or an atrial extrasystole?
2. + 3. after one comes to the conclusion that it is a sinus node P: why is it not conducted and why is the PP distance smaller when there is a QRS complex in between than when there is not.
Regarding 1: There could also be an atrial extrasystole. The closer to the sinus node this arises, the more similar it is to the sinus node P (roughly speaking). All P waves look identical here, which indicates that they are all sinus node Ps. Everything would be simpler in a 12-lead ECG!
2. Every 2nd P wave is not conducted because the conduction system (here most probably the AV node) is refractory due to the preceding PVC (condcealed conduction: the VES penetrates retrogradely at least partially into the AV node and makes it temporarily refractory).
3. There is a ventriculophasic sinus arrhythmia, which explains the cyclically changing PP intervals. Several mechanisms have been proposed for ventriculophasic sinus arrhythmia: phasic changes in baroreceptor mediated vagal input to the sinus node, mechanical effects and pressure changes caused by ventricular systole, and increased blood flow to the sinus node.
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.