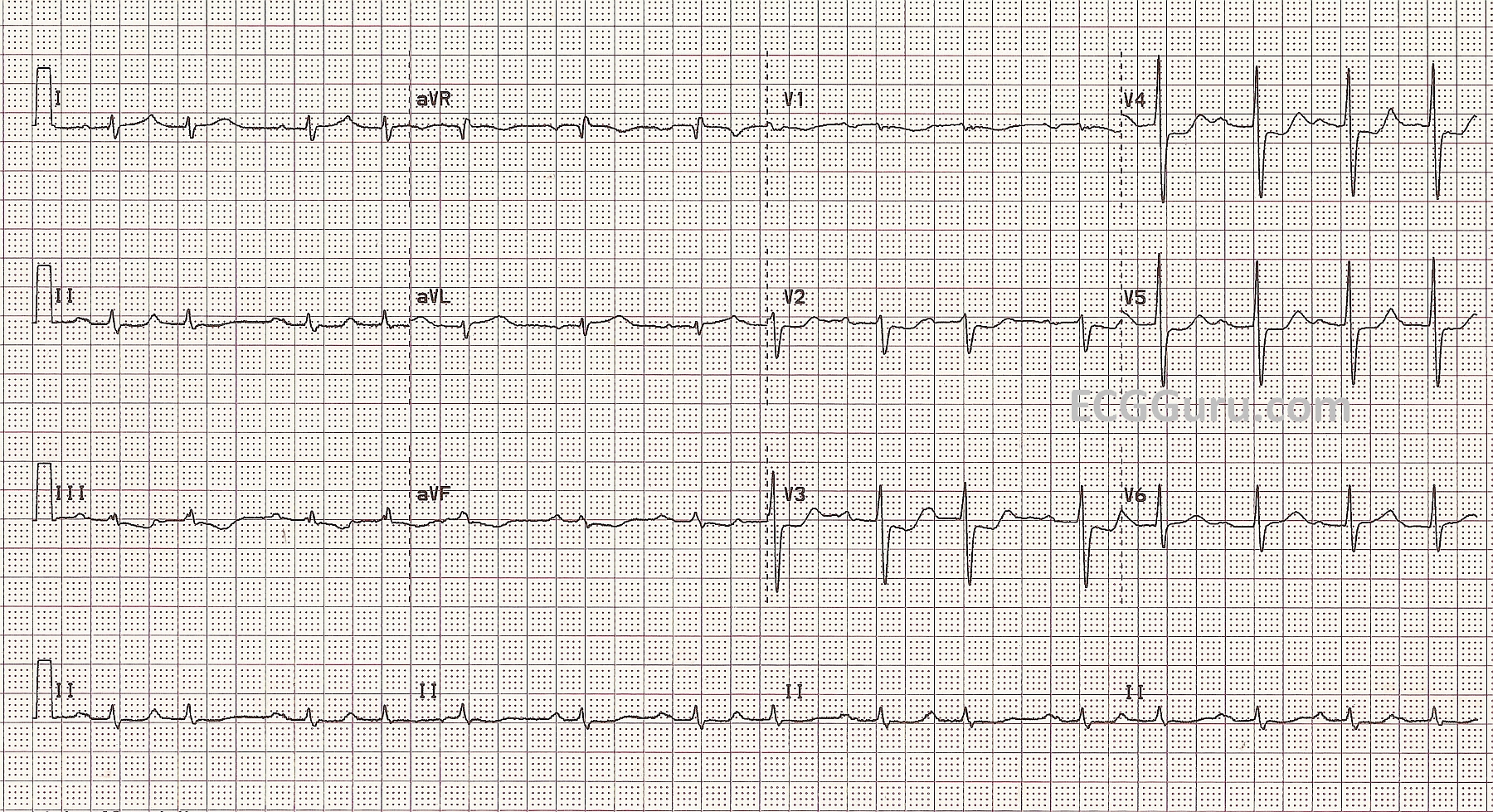
This ECG illustrates what some would call a non-ST-elevation M.I., but may also illustrate the limitations of a standard 12-Lead ECG. This female patient in her 60's presented to the Emergency Department with vague chest discomfort. She was cool and diaphoretic. She gave a history of having coronary artery stents placed in the past. On angiography in the cath lab, she was found to have two stents in her obtuse marginal artery which were occluded. Her case was lost to followup.
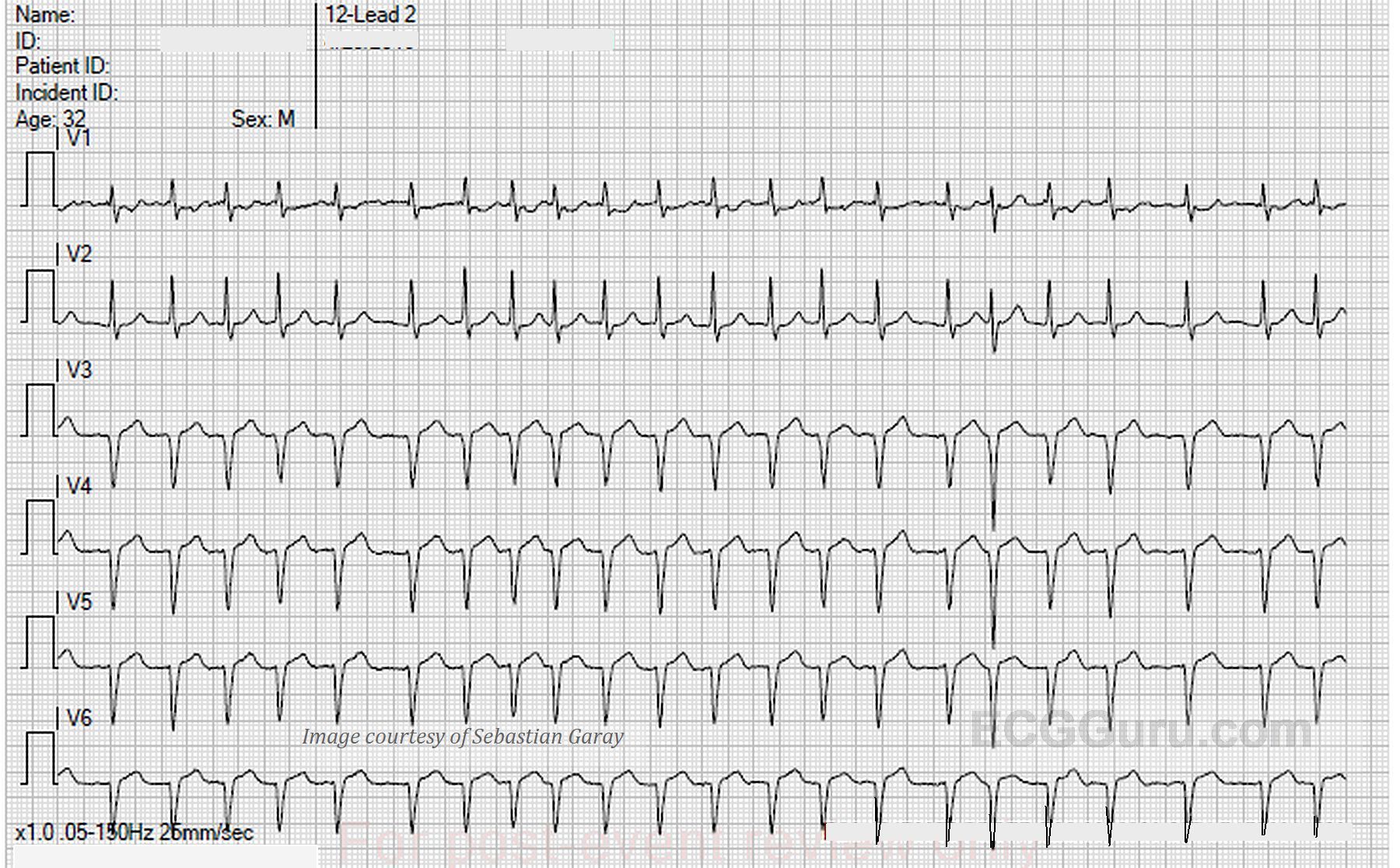
The ECG shows ST depression in anterior leads V2 through V6, as well as in the inferior leads, although very subtle. The inferior leads' ST segments are more horizontal than depressed, but flat and horizontal is not normal. She shows a bit of upward concavity or slight elevation in V1, Lead I, and aVL. These signs might be missed by someone looking only for ST ELEVATION. Additional left lateral and posterior leads were not done, and we have to wonder if she would have had some ST elevation in V7 or V8.
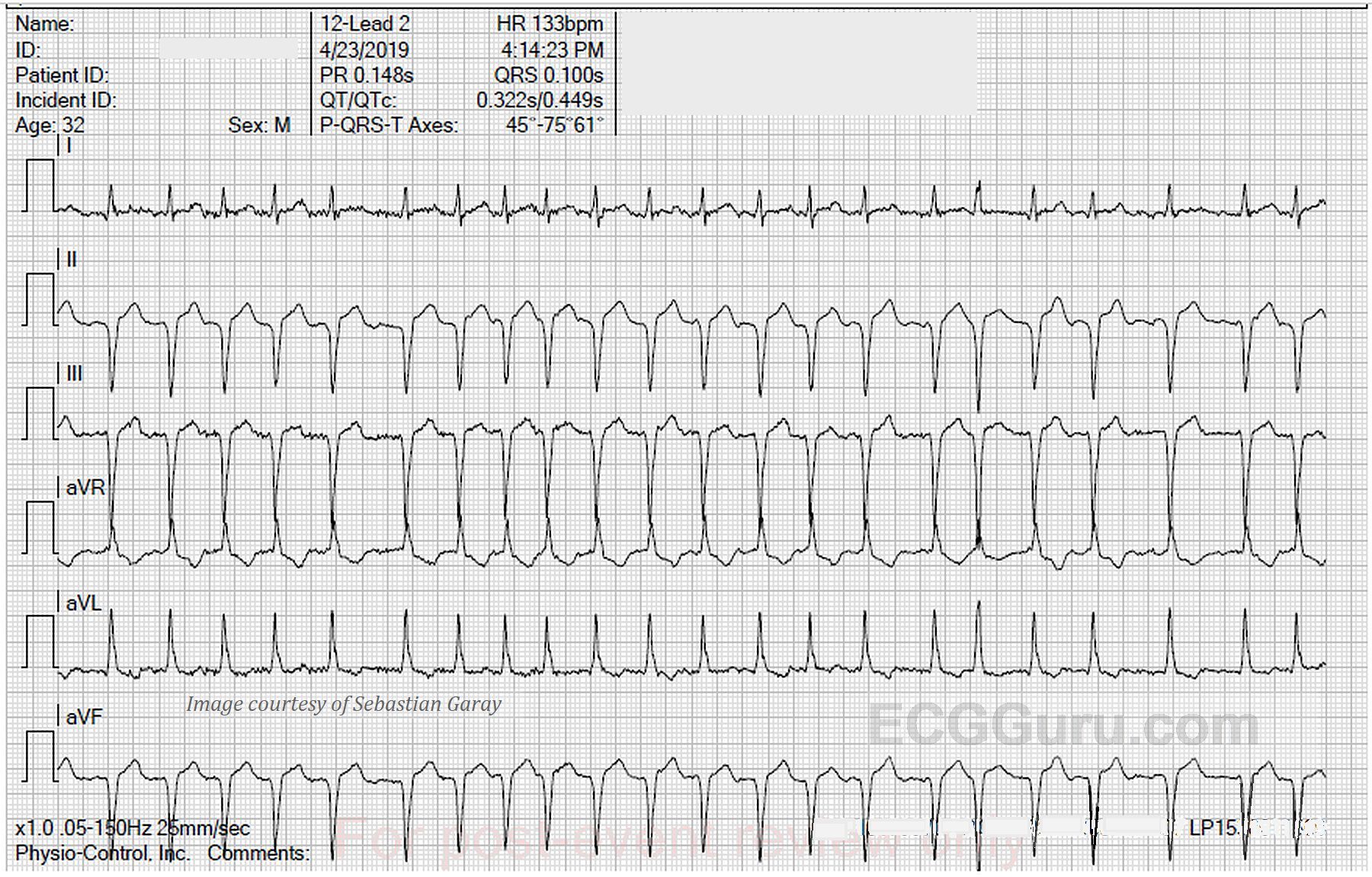
Her rhythm is very interesting too. Often, ischemic hearts produce abnormal rhythms, and it is not unexpected. The rate and the rhythm caused this patient no difficulties during her time in the ED. On first glance, her QRS complexes appear to be "grouped", as they would in a Wenckebach type block. On closer inspection, you will see two distinctly different P waves, and no non-conducted P waves. This appears to be a sinus rhythm with frequent PACs. The PRI is prolonged at .28 sec., which also is not unusual for M.I. patients.
We are very interested to hear what YOU think about this interesting ECG, including the rhythm. We are hoping to hear from people from all areas of cardiac care - what do you think are the main teaching points of this case?