The Patient This ECG was recorded from an 86-year-old man who was weak, pale, and diaphoretic. He was hypotensive, with a BP of 88/54. He denied chest pain or shortness of breath.
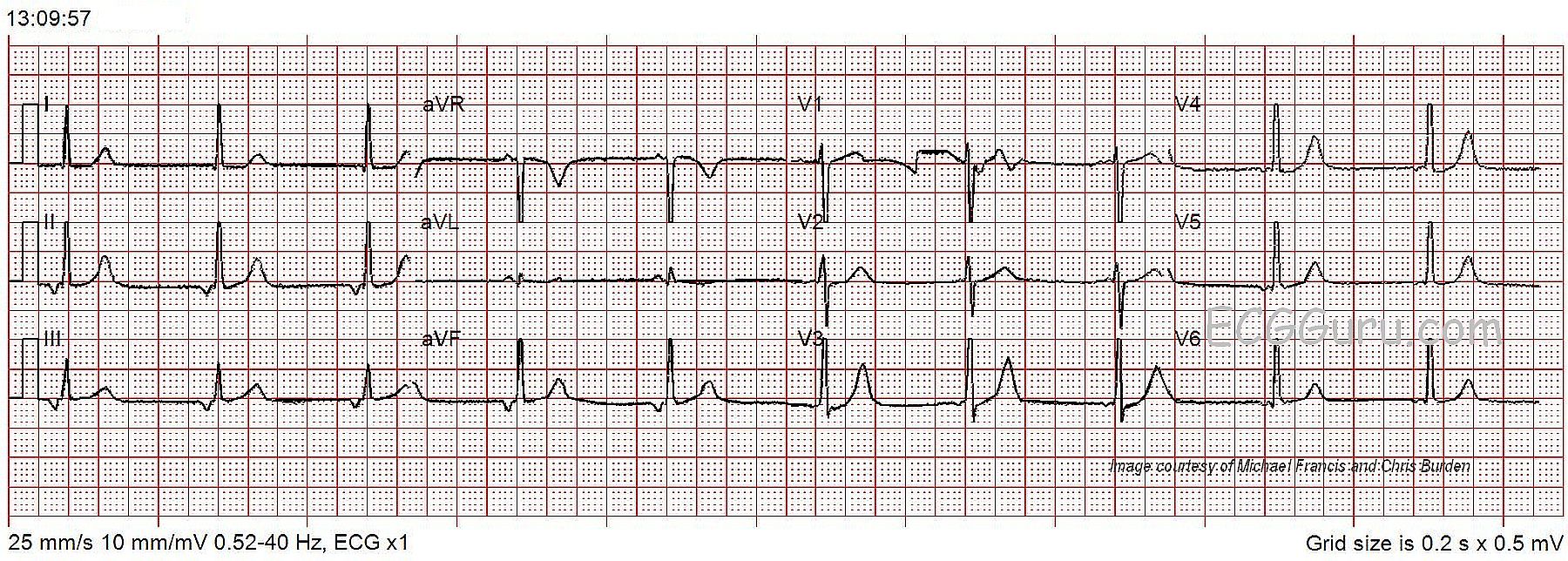
The ECG The 12-lead ECG shows a bradycardia at about 60 beats per minute and regular. The QRS complexes are narrow, at a little less than .08 seconds (800 ms). The P waves are negative in Leads II, III, and aVF and positive in aVR. This is an indication that the P waves are traveling in a “retrograde” fashion – backward. The origin of the P waves has to be the AV junction or the lower atria for this to happen. The PR interval is on the short side of normal at about .12 seconds (120 ms), possibly even less. This is common in junctional rhythm, as the impulse starts at the AV junction, and travels back through the atria and forward through the ventricles at the same time.
There are no premature beats, and the ST segments are not elevated or depressed. There are no T wave inversions, except for aVR, where it is normal.
Assessment One cause of junctional rhythm is sinus brady. That is, the sinus node begins firing so slowly that the junctional pacemaker “escapes”, and takes control of the heart. When the sinus node speeds up, it may once again take over the heart’s rhythm from the junction. The fastest pacemaker controls the heart. A junctional rhythm may escape when the sinus node fails or there is a complete AV block in the AV node area.
Patient Outcome This patient was diagnosed with orthostatic hypotension, bronchitis, and urinary tract infection. He was treated in the hospital and cleared by a cardiologist for discharge two days later.
Our thanks to Michael Francis and Chris Burden for donating this ECG.