Thank you to Alikuni Kllany from Toronto for donating these ECGs. They are from a 59-year-old man who has a history of hypertension and depression. Last year, he was on atenolol when he experienced a brief syncopal episode and bradycardia. He was taken off atenolol and started on amlodipine 5 mg. He also takes ramipril 10 mg, atorvastatin 40 mg, and tamsulosin .4 mg. He continues to have bradycardia and dizziness.
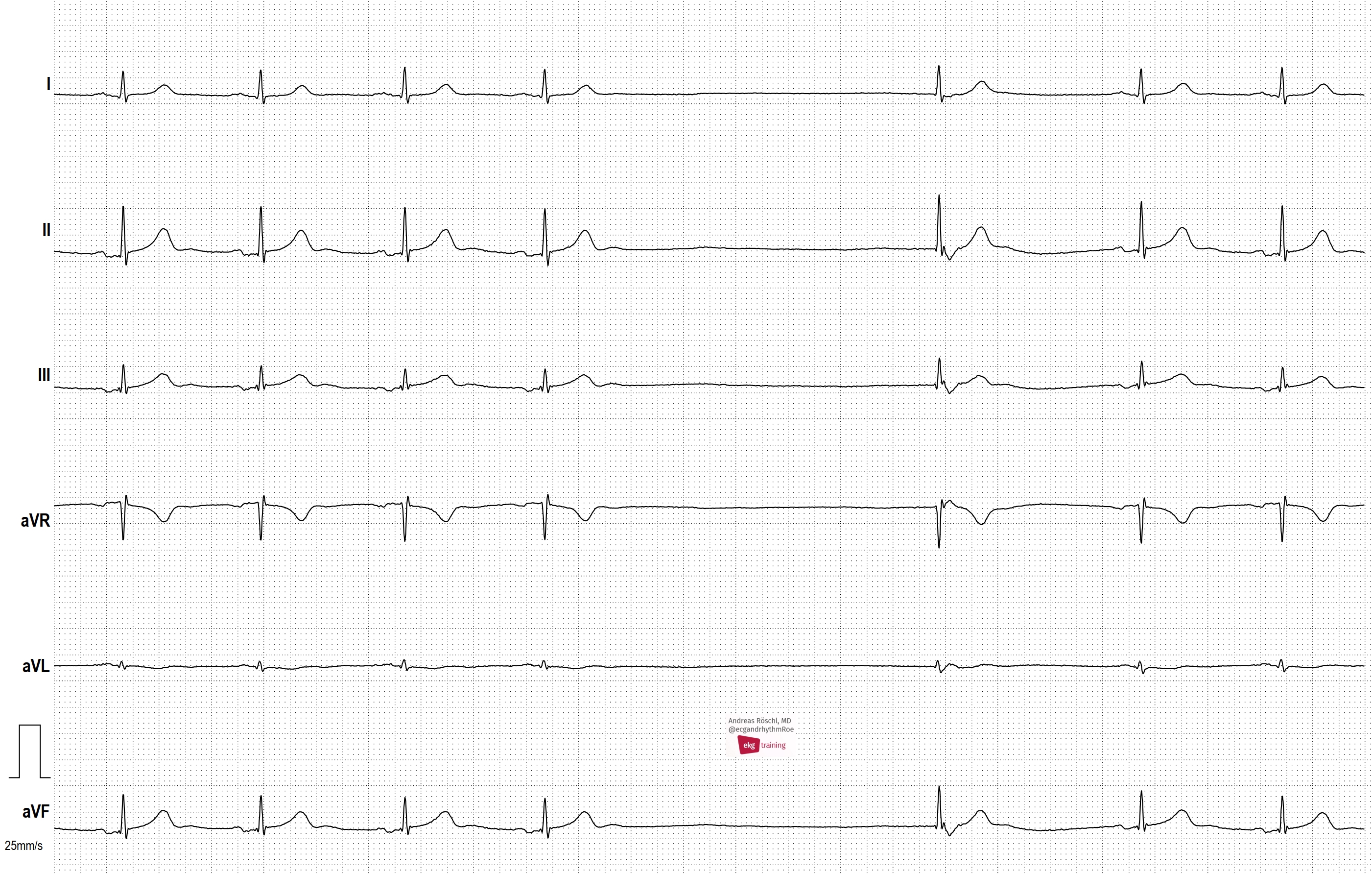
The first ECG shows grouped beating, with repetitive groups of two and three complexes. The P waves are very small, and hard to evaluate. The best place to see them is in the Lead II rhythm strip at the bottom. The rhythm strip is not run concurrently with the 12-Lead, making it even more difficult to evaluate P wave morphology.
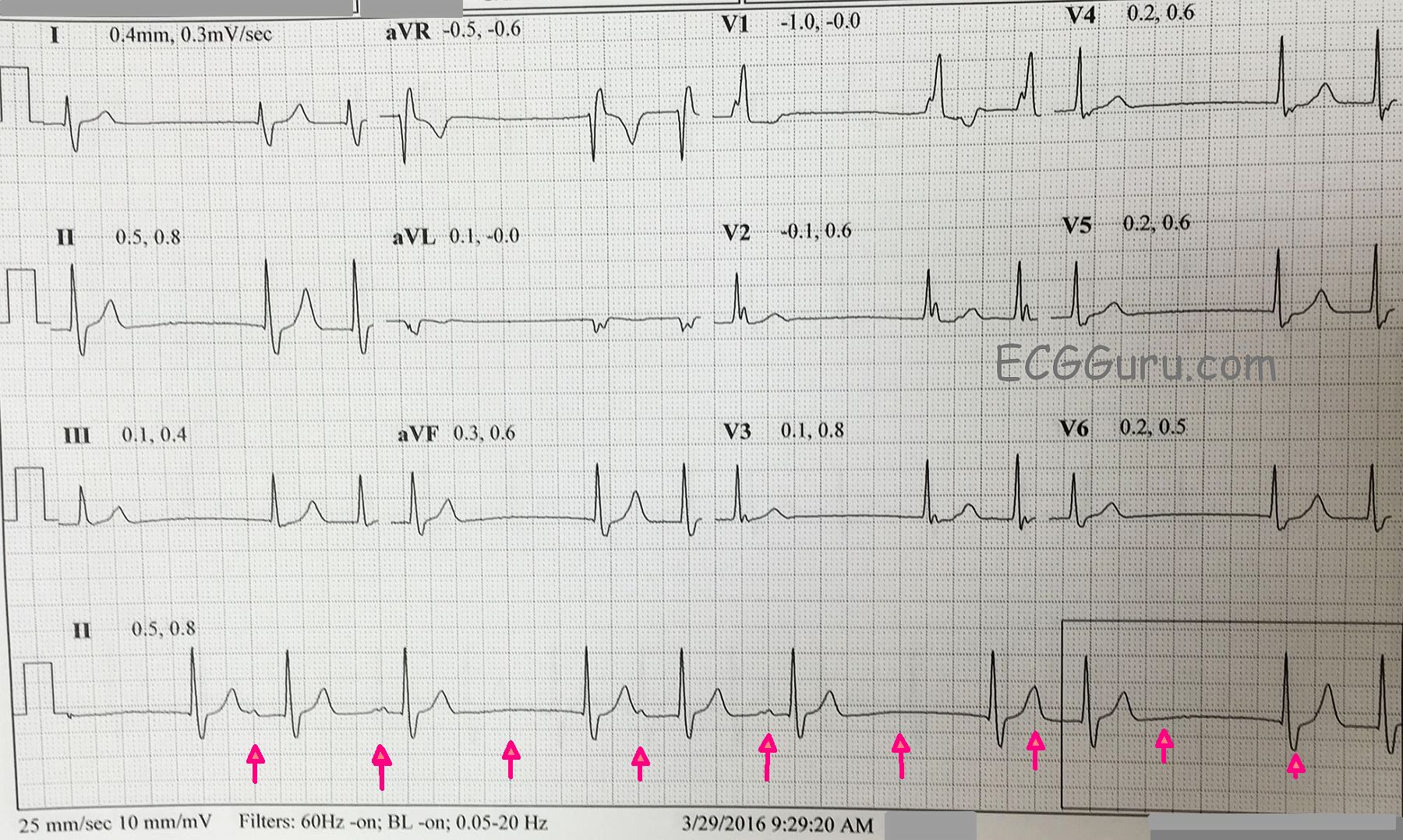
The beats that begin the groups also END a pause. These are junctional escape beats. After the junctional escape beats, the PR intervals vary. This can be explained by RP / PR reciprocity, first described by Mobitz. He demonstrated that the RP interval can affect the next PR interval. Longer RP intervals (slower rate) cause PR shortening. Shorter RP intervals equal longer PR intervals. The P waves are so small, it is difficult to determine whether there is a P wave in the last T wave of each group, which would indicate non-conducted PACs. So, we are left with a sinus pause or sinus exit block (suggested by the timing of the first six beats. We have used red arrows to suggest where the sinus node probably fired. P waves indicate conduction, of course. Lack of P waves, the impulse failed to exit the sinus node.
There are many mechanisms by which grouped beating can occur. Second-degree AVB, Type I (Wenckebach) comes to mind first. That rhythm in it’s pure form would have a regular sinus rhythm underlying it. Escape-capture bigeminy often occurs with slow rates and junctional escapes, but does not by itself cause “trigeminy”. Sick sinus syndrome can cause all types of chaos in the rhythm.