Today's expert is Jason E. Roediger, CCT, CRAT, who is a highly respected Cardiovascular Technician at the Dept. of Veterans Affairs, Hunter Holmes McGuire VA Medical Center in Richmond, VA. He is known for holding numerous certifications in all levels of ECG interpretation, and also for scoring 100% on the Level IV Advanced ECG Board Certification exam that is usually reserved for cardiologists.
Answer: Always? No. Usually, Yes.
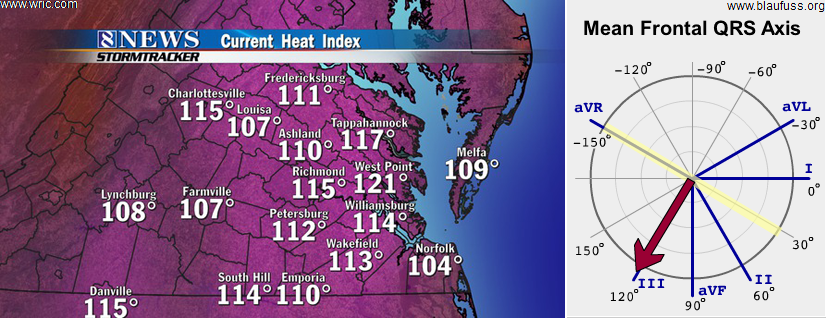
There are exceptions to several "golden rules" in electrocardiography and this one is not exempt. One of the chronic issues contributing towards widespread confusion in understanding electrical axis is a lack of continuity in terminology. There is no general concensus on how to refer to an axis in the right upper quadrant. Depending on which author you are reading, it has traditionally been known by multiple names: Northwest axis. . . upper right quadrant. . . extreme right axis. . . right superior axis. . . "no-man's-land" (i.e., "N-M-L".). . . etc. Because my first exposure to electrical axis was through Dr. Marriott's textbooks and he prefered to use "N-M-L", I have personally latched on to that particular name as well. Even though some persist in calling it an "extreme left axis" or "far left axis deviation", this practice is frowned upon and discouraged. It's important to note that an axis in "N-M-L" is not synonymous with an "indeterminate" axis which occurs when the QRS is essentially isodiphasic or equphasic in all 6 limb leads and therefore the polarity of the QRS cannot be discerned in leads I and aVF.
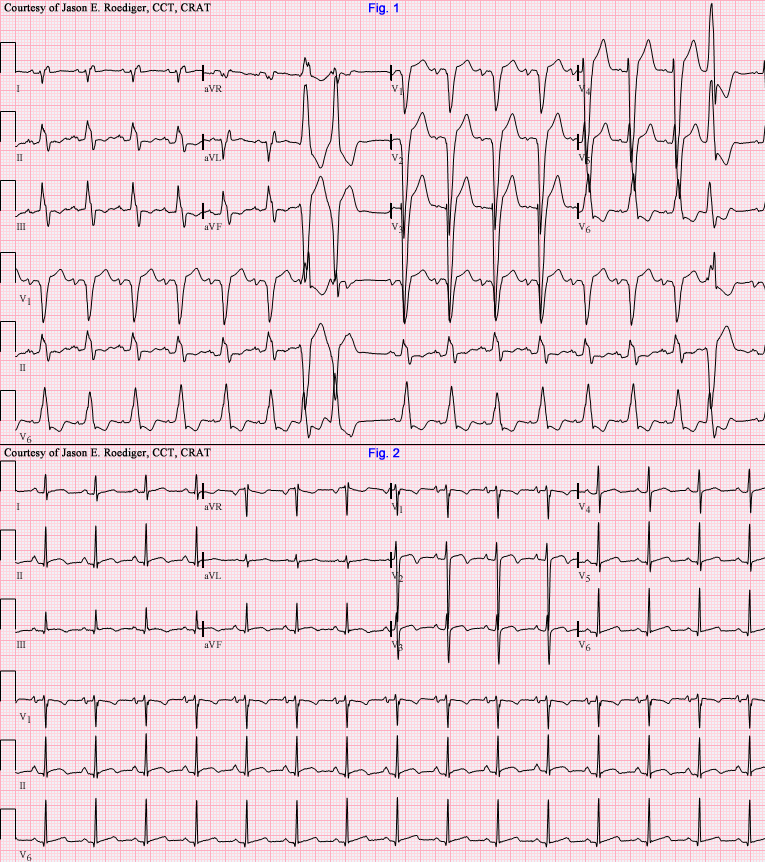
Definition: An axis in "N-M-L" is recognized when the QRS complex has a predominantly or wholly negative deflection (i.e., down) in leads I and aVF. The axis is −90 to −180 degrees.
Irregardless of which descriptive name you prefer, in the context of a wide QRS complex tachycardia, this particular axis is highly predictive of ventricular tachycardia and is rarely encountered in "conducted" rhythms however some examples of aberrant SVT have been published with an axis in "N-M-L".
In summary: An axis in "N-M-L" implies (but is not proof of) an apical origin to the rhythm and should make one think of and exclude the possibility of ventricular tachycardia. As a general rule, until it is proven otherwise, assume any wide QRS complex tachycardia is ventricular tachycardia. Even though this one clue carries significant weight in supporting the interpretation of ventricular tachycardia, that conclusion can not be made based solely on this single criteria. This axis is just one of a long list of criteria and should be used in conjunction with all of them as they carry alot of strength when used collectively.