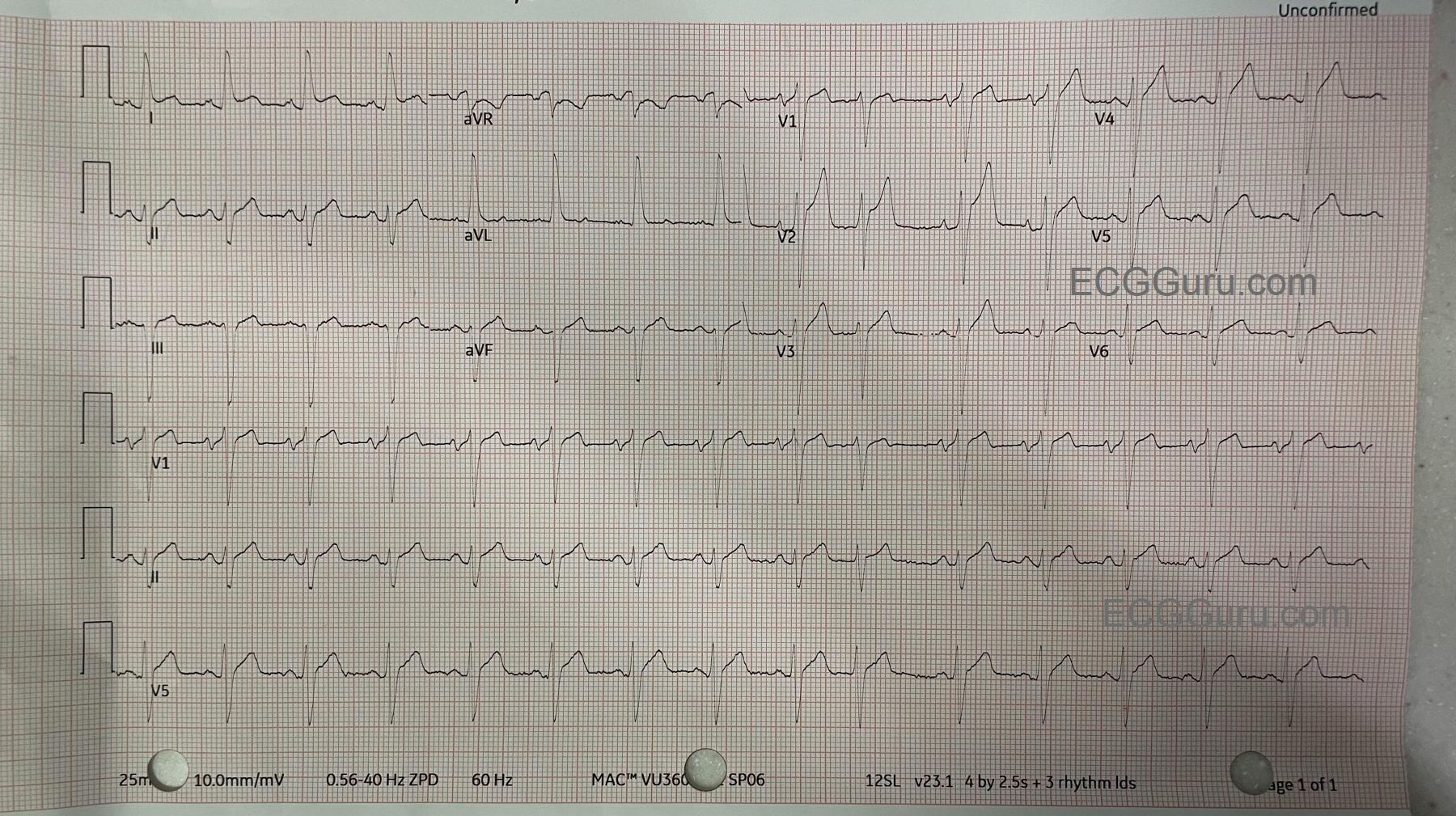
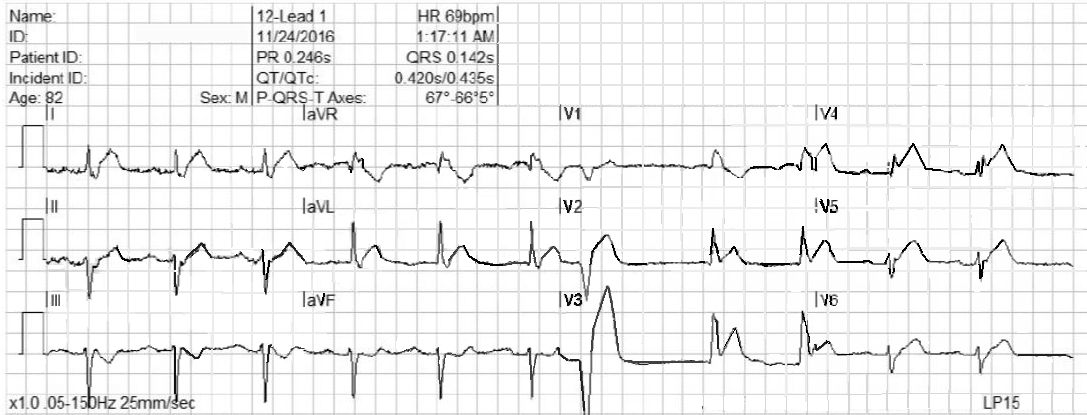
This ECG is taken from an 82-year-old man who called 911 because of chest pain. He has an unspecified “cardiac” history, but we do not know the specifics.
WHAT IS THE RHYTHM? The heart rate is 69 bpm, and there are P waves before every QRS complex. The underlying rhythm is regular, with one premature beat that is wide without a P wave. The PR interval is slightly prolonged at .25 seconds. The rhythm is normal sinus rhythm with first-degree AV block and one PVC.
WHY THE WIDE QRS? The QRS complex is wide at .14 seconds. The QRS in V 1 has a wide R wave after a small Q wave. This in consistent with right bundle branch block pattern, with loss of the normal initial small r wave (pathological Q waves). The diagnosis of RBBB is further corroborated by the wide little S waves in Leads I and V6. The QRS frontal plane axis is -66 degrees per the machine, and clearly “abnormal left” because the QRS in Lead II is negative, while the QRS in Leads I and aVL are positive. This is left anterior fascicular block, also called left anterior hemiblock. The combination of RBBB and LAFB is a common one, as the two branches have the same blood supply. It is also called bi-fascicular block.
WHAT ABOUT THE ST SEGMENTS? The ST segments in leads V2 through V6 are elevated, and their shape is very straight, as opposed to the normal shape of coved upward (smile). Even though the amount of ST elevation at the J points appears subtle, the shape of the segments, the fact that they appear in related leads, and the fact that the patient is an elderly male with chest pain all point to the diagnosis of ANTERIOR WALL ST elevation M.I. (STEMI). Additional ST changes include a straight shape in Leads I and aVL and ST depression in V1 and aVR.
PATIENT OUTCOME The patient was transported to a cardiac center, where he received angioplasty in the cath lab. The left coronary artery was found to be occluded, and was repaired and stented. He recovered without complications and was sent home in a few days.