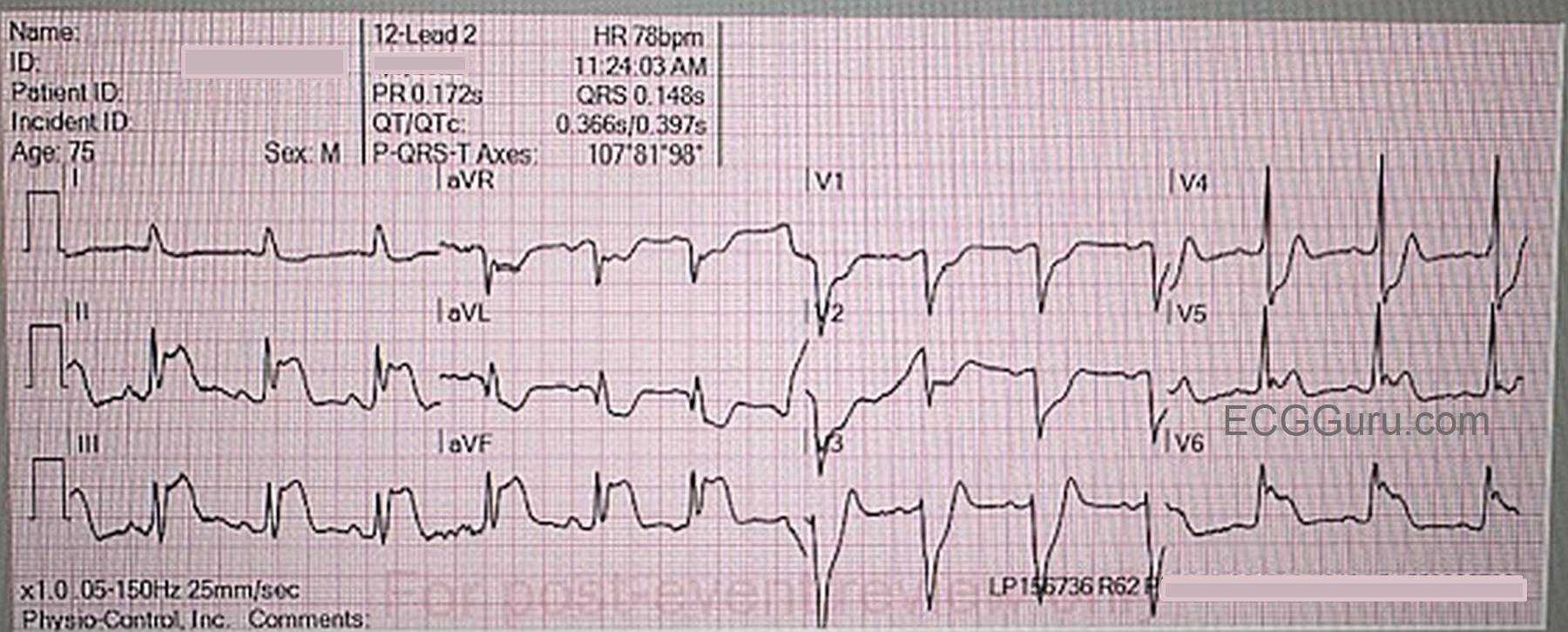
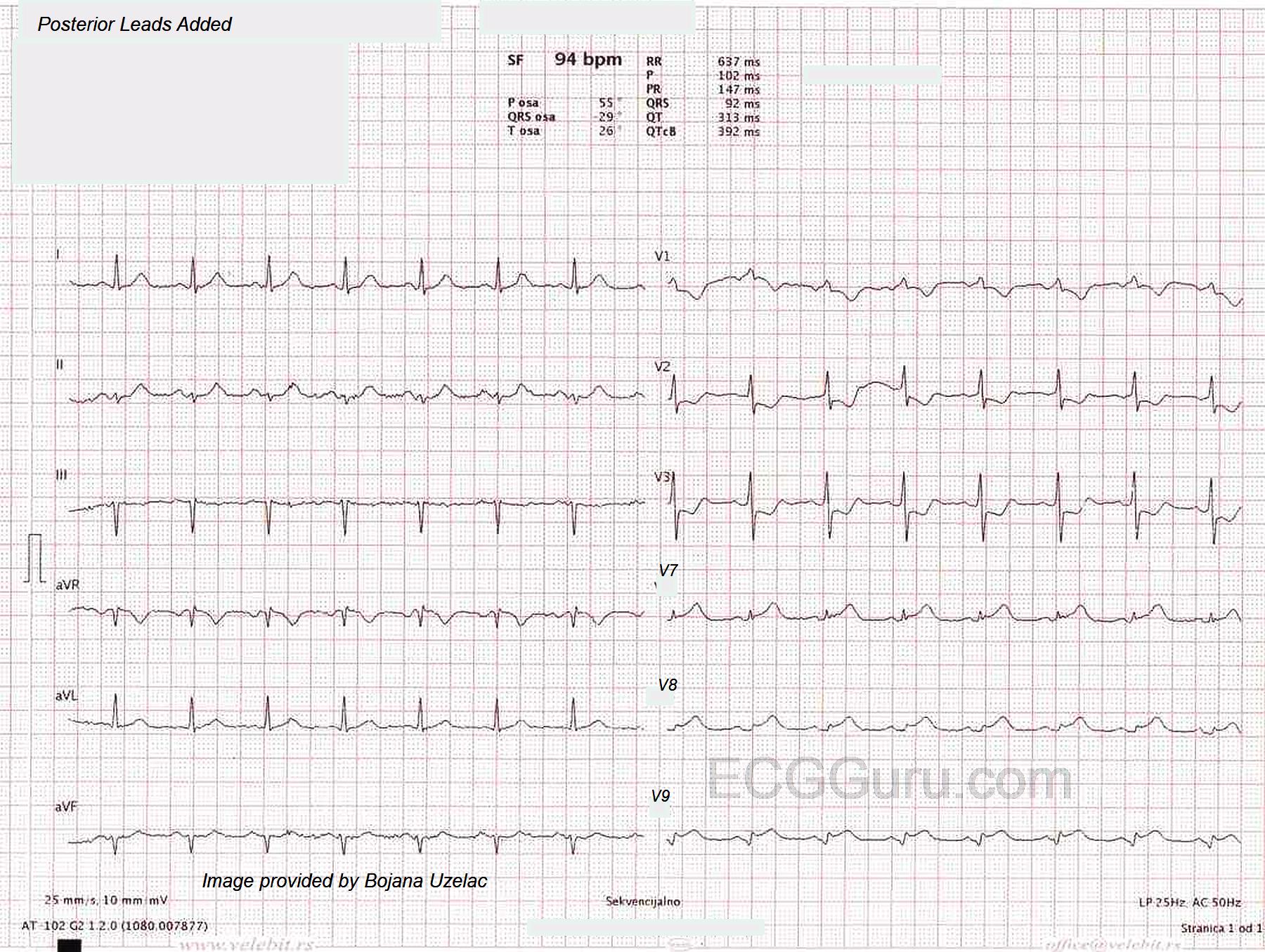
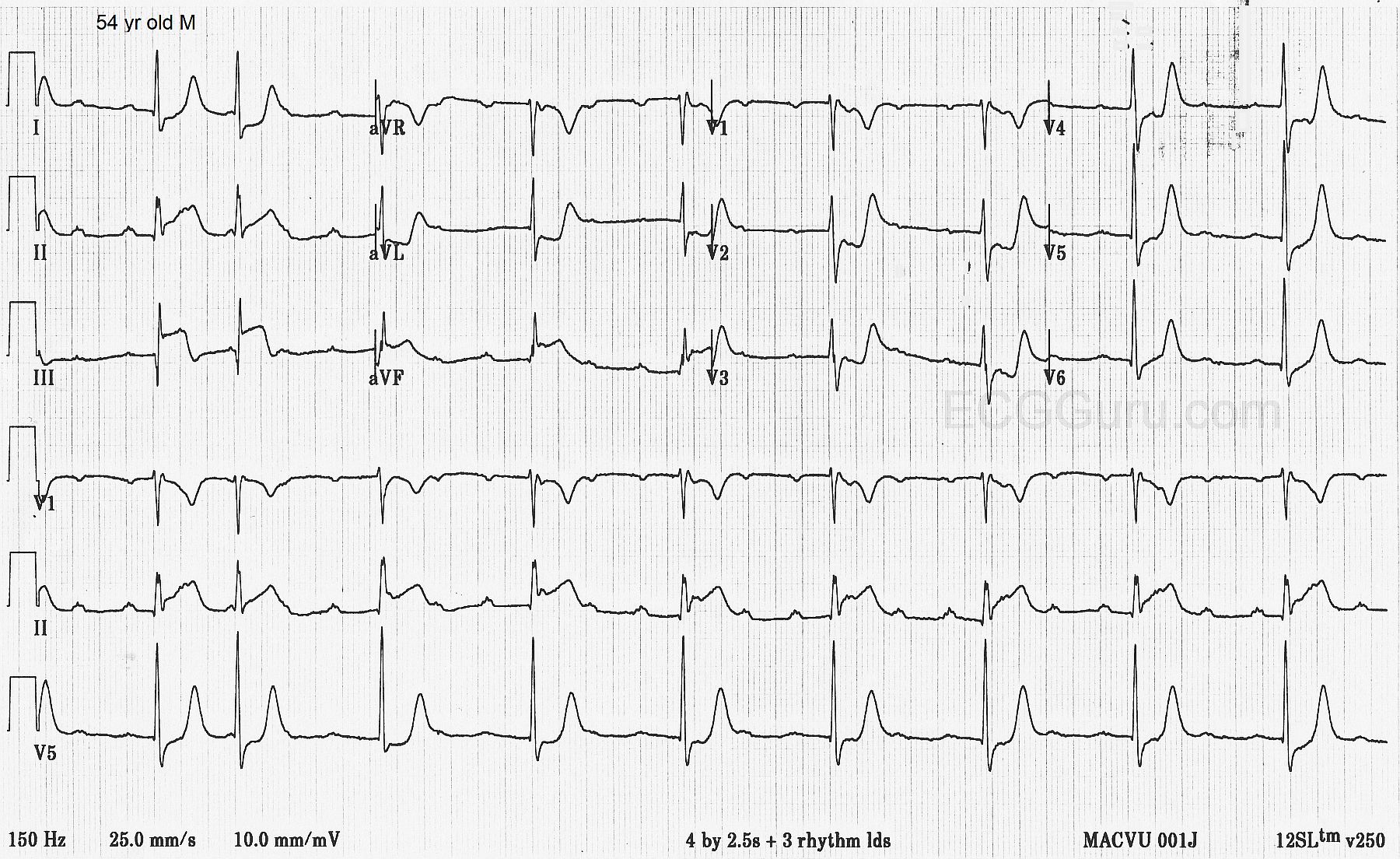
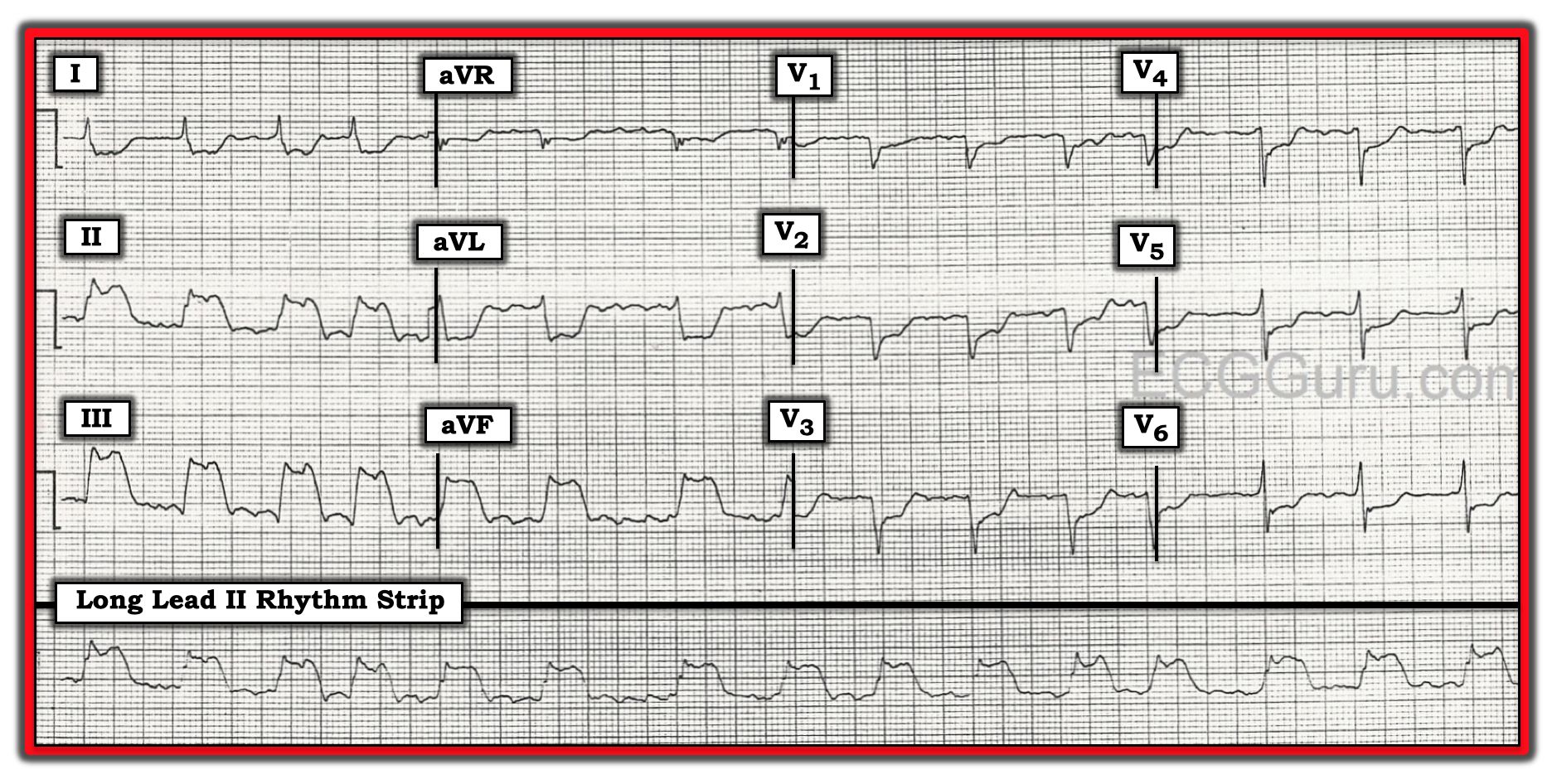
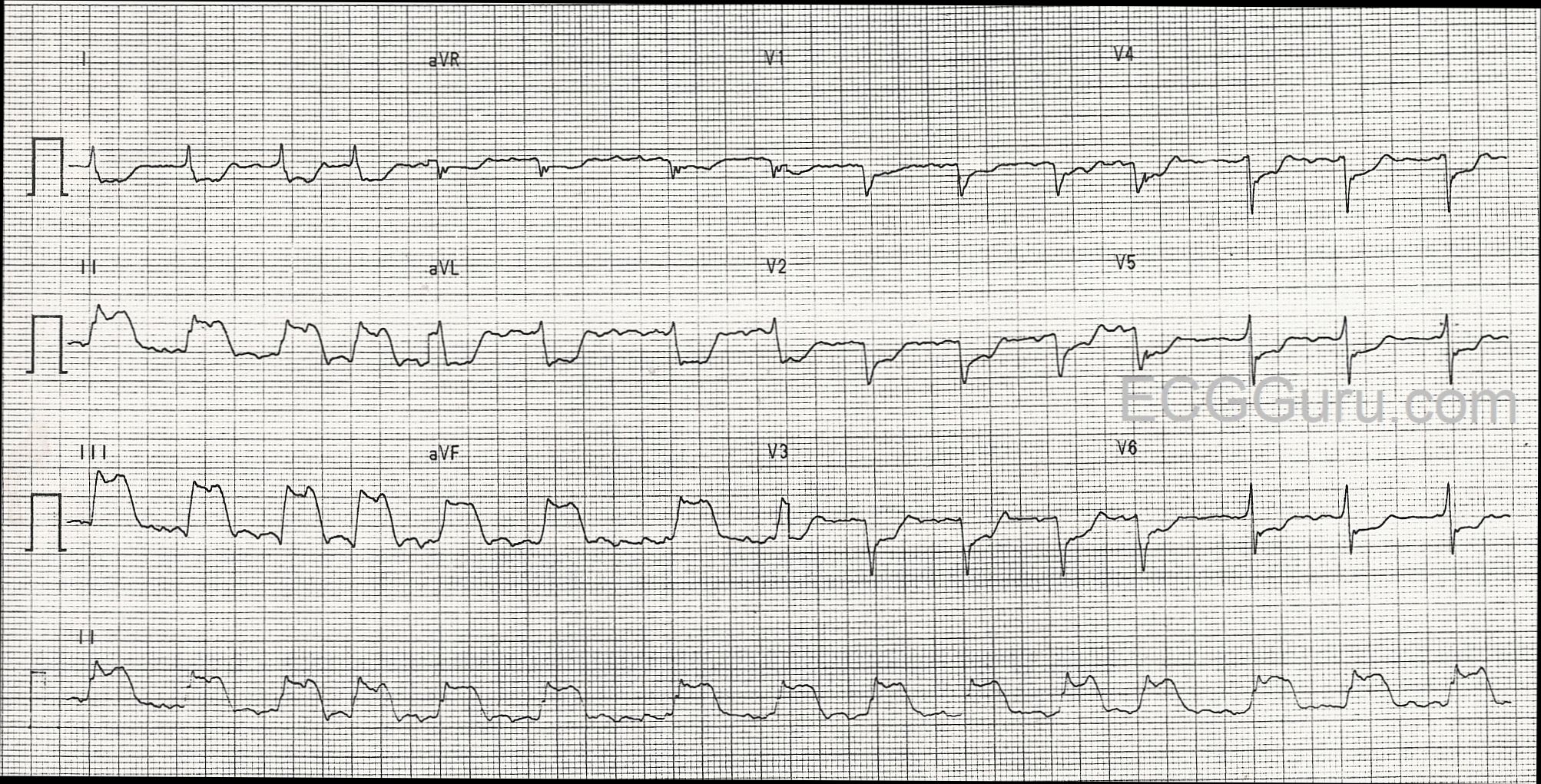
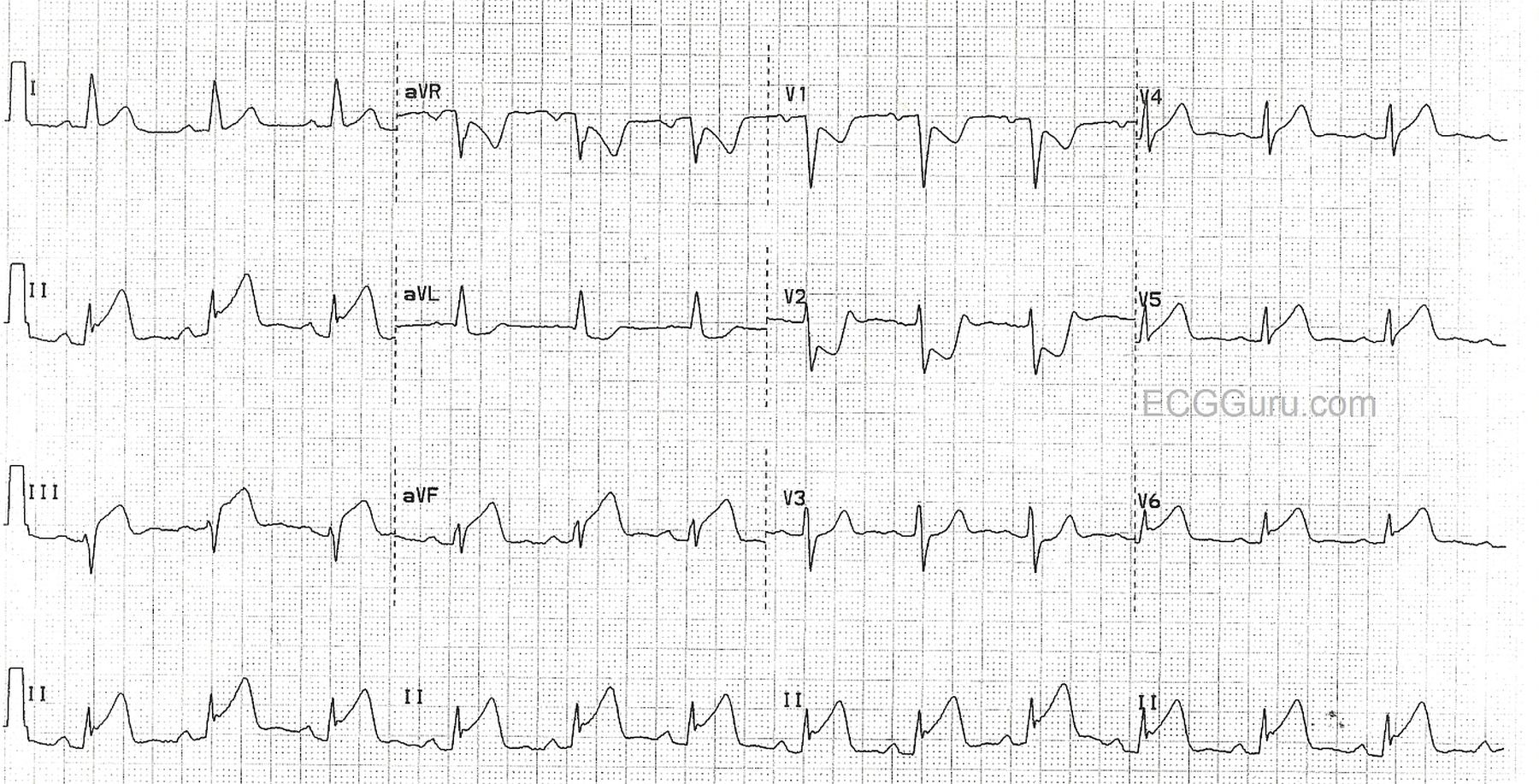
This is from a Cardiac Alert patient, with chest pain, in the Emergency Department. The ECG shows ST elevation in the inferior leads (II, III, and aVF), and in the low lateral leads (V5 and V6). There is reciprocal depression in V1 and V2, indicating injury in the posterior wall. One could argue that "inferior" is just the term we use for the lower part of the posterior wall - the part that faces the floor in a standing person. So, "inferior-posterior" reflects a more proximal occlusion of the culprit artery.
The high lateral wall is represented by I and aVL. These leads would usually show marked reciprocal ST depression when II, III, and aVF have elevation. However, in this ECG, aVL is depressed, but not as much as expected, and Lead I almost looks elevated! This could represent even more extensive lateral wall involvement. A dominant right coronary artery could be the culprit, but it seems more likely that a dominant circumflex artery is to blame, as it could perfuse the entire lateral wall before joining with the posterior descending artery and perfusing the inferior wall. Unfortunately, we do not have the cath results on this patient.
The ST elevation in this ECG has the classic appearance of acute M.I., and will be interesting to both beginner and advanced students.
Often, one ECG can provide a wealth of teaching opportunities, no matter what the level of your students. For the student learning to monitor the rate and rhythm, you might crop this image to only show the Lead II rhythm strip at the bottom, for a good example of normal sinus rhythm with a borderline PRI of .20 sec. For the student learning about ST elevation M.I., this is a good example of inferior-posterior and lateral injury. Leads aVL, V1 and V2 demonstrate reciprocal ST depression. When an observant student notices the slight ST elevation in V6, a discussion of coronary artery distribution can occur.