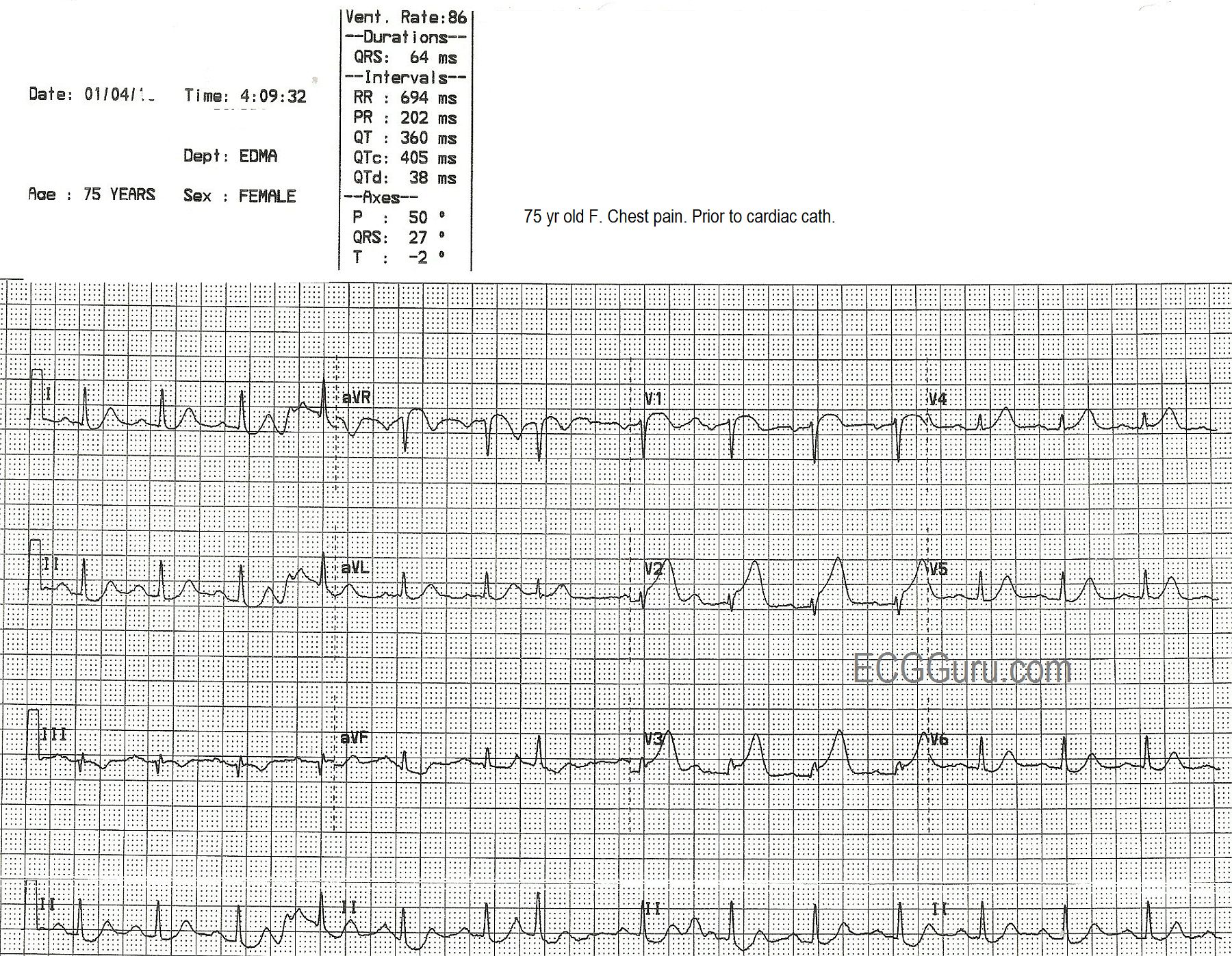
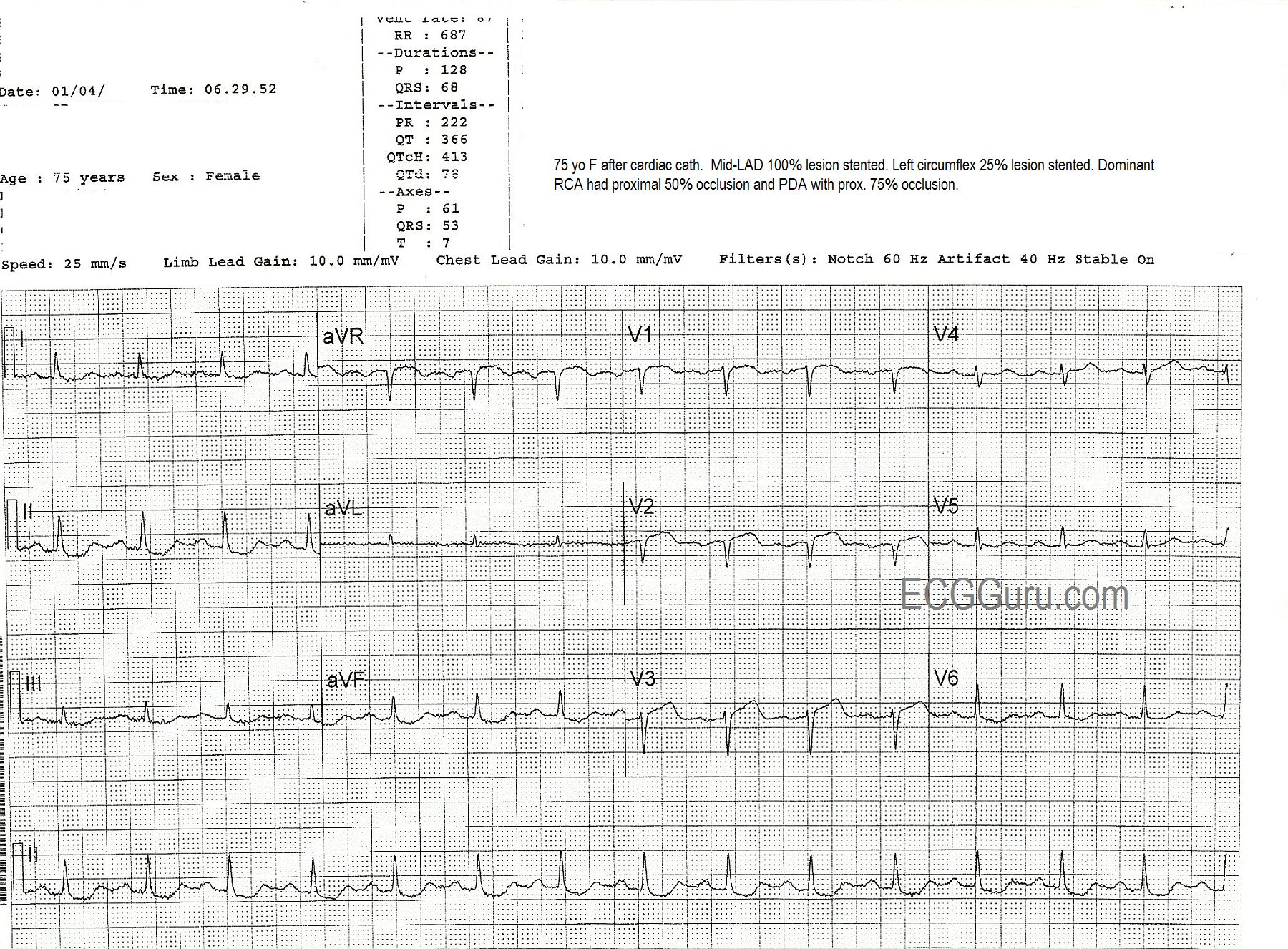
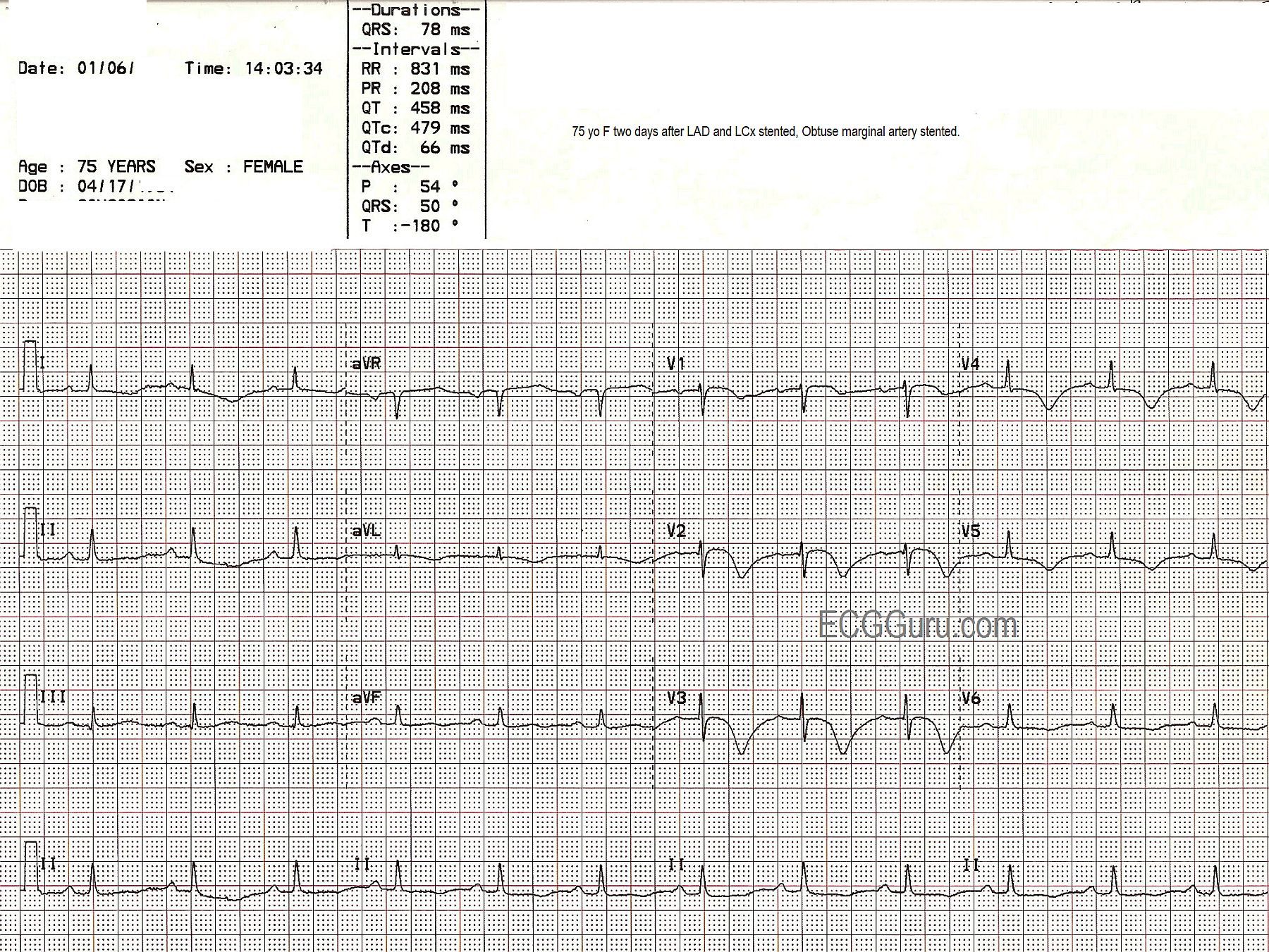
This series of three ECGs is from a 75-year-old woman who came to the Emergency Dept. with chest pain. The first ECG shows ST elevation in V1, V2, and V3, with generally low voltage in the QRS complexes. There is some coving upward of the ST segment in aVR, which can suggest a very proximal lesion of the left coronary artery (LCA). She was taken to the cath lab, where it was discovered that she had a 100% occlusion of the midportion of the anterior descending branch of the left coronary artery, which was repaired and stented. The second ECG, taken after the angioplasty, shows some Q waves in V1 and V2, with poor R wave progression in the V leads. A 25% occlusion of the obtuse marginal branch of the circumflex artery was stented two days later. The third ECG was obtained after that procedure. It shows that the Q waves have disappeared in the anterior leads (possibly due to different technicians performing the ECGs with different lead placement). It also shows marked T wave inversion in I and aVL, representing ischemia in the lateral wall, and in all the chest leads, representing ischemia in the anterior wall. The QTc is prolonged in this third ECG at 479 ms. It is not known what medications the patient was on. This patient also had a 50% proximal occlusion in the RCA and a 75% occlusion in the posterior descending artery. This is a good example of a patient with extensive coronary artery disease who finally presented for treatment when she developed ST elevation M.I.