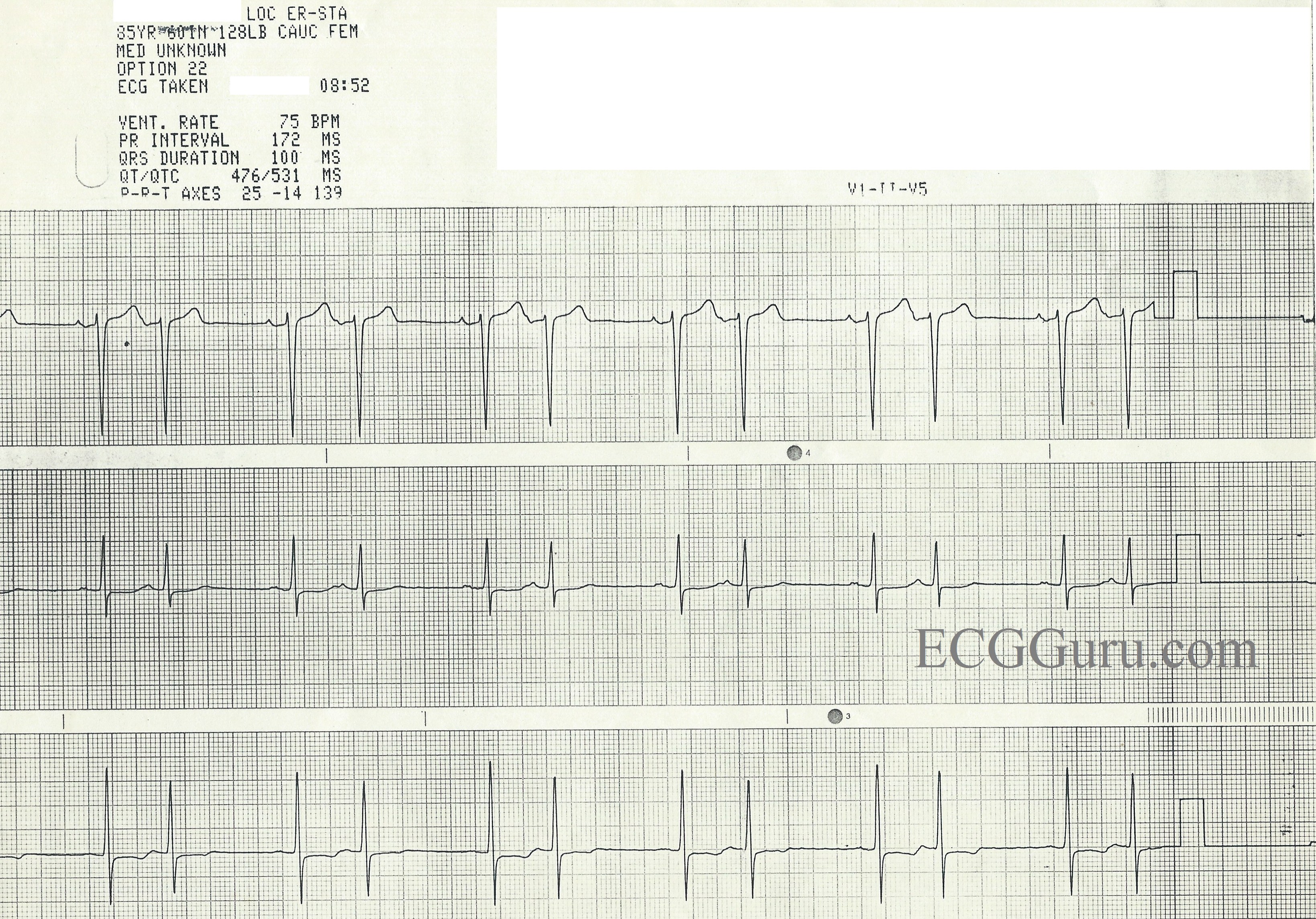
This three-lead rhythm strip is from an 85 year-old-woman for whom we have no other information, unfortunately. It shows an obvious, regular bigeminal pattern. There are many rhythms that can cause bigeminy, with regular, paired beats. So, how do we analyze this rhythm?
First, we can see that all the QRS complexes are fairly narrow and look alike in each lead. So, we know this is a supraventricular rhythm. The rhythm “marches out”, with the same spacing between all the paired beats, and exactly one P-QRS missing after each pair.
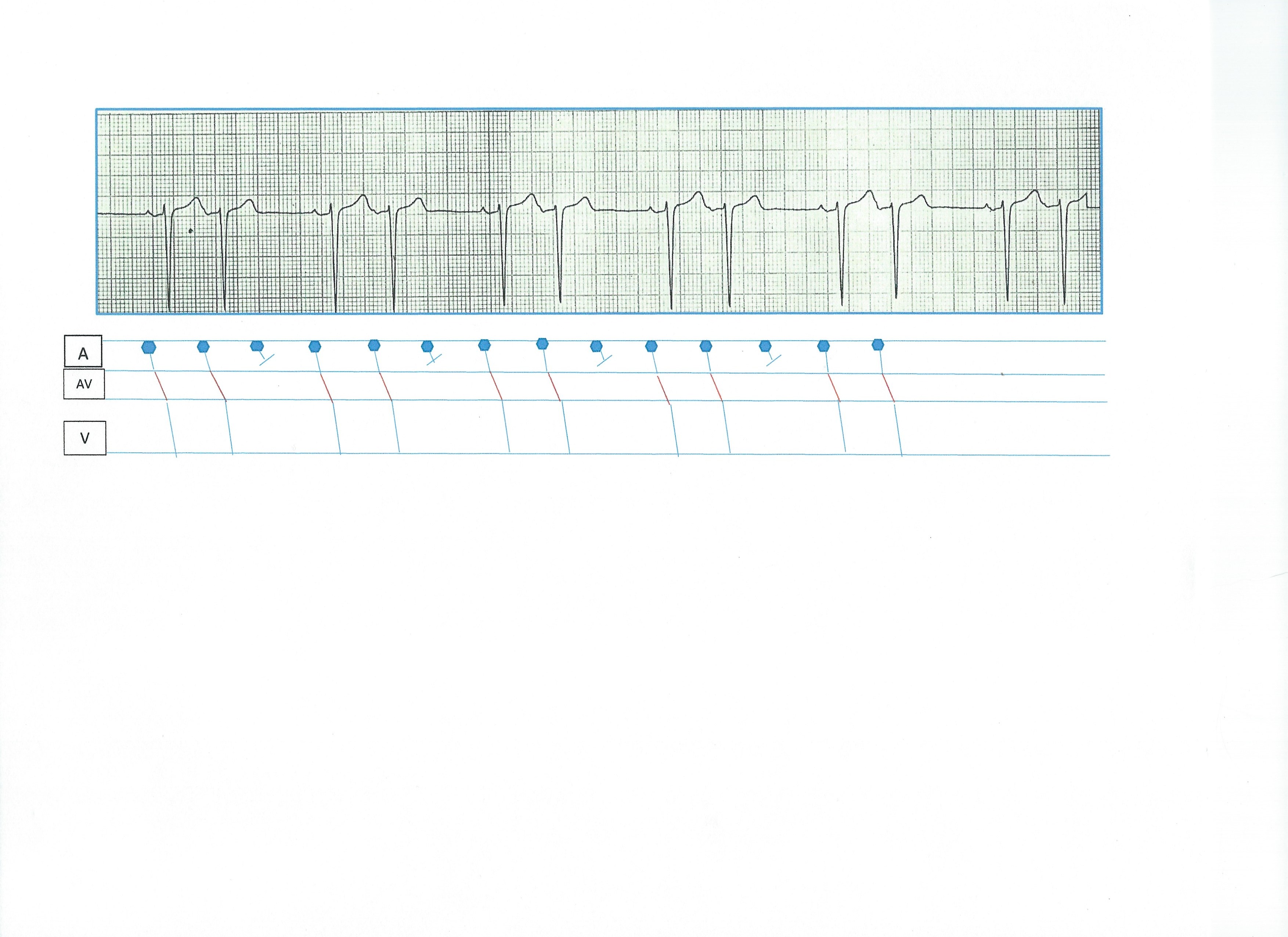
Sino-atrial exit block occurs when the sinus node fires, but the impulse is unable to exit the sinus node. No P wave will occur, but the sinus node continues to fire in a regular rhythm. There are four types of SA block, just as there are four types of AV block. This ECG meets the criteria for a Second-degree, Type II SA block.
First-degree SA block would not be decipherable on the ECG, as we do not see the SA node fire, and therefore cannot measure an interval between the SA node firing and the production of a P wave.
Second-degree SA block, Type I would have progressively prolonging exit times for the impulse leaving the SA node. This would produce progressively shortening R-to-R intervals, until the pause.
Second-degree SA block, Type II has regular R-to-R intervals until the pause, and the pause will equal two or more (usually two) R-to-R intervals.
Third-degree SA block produces NO P WAVES, and would have to be diagnosed on electrophysiology studies, as it would usually result in a junctional escape rhythm.