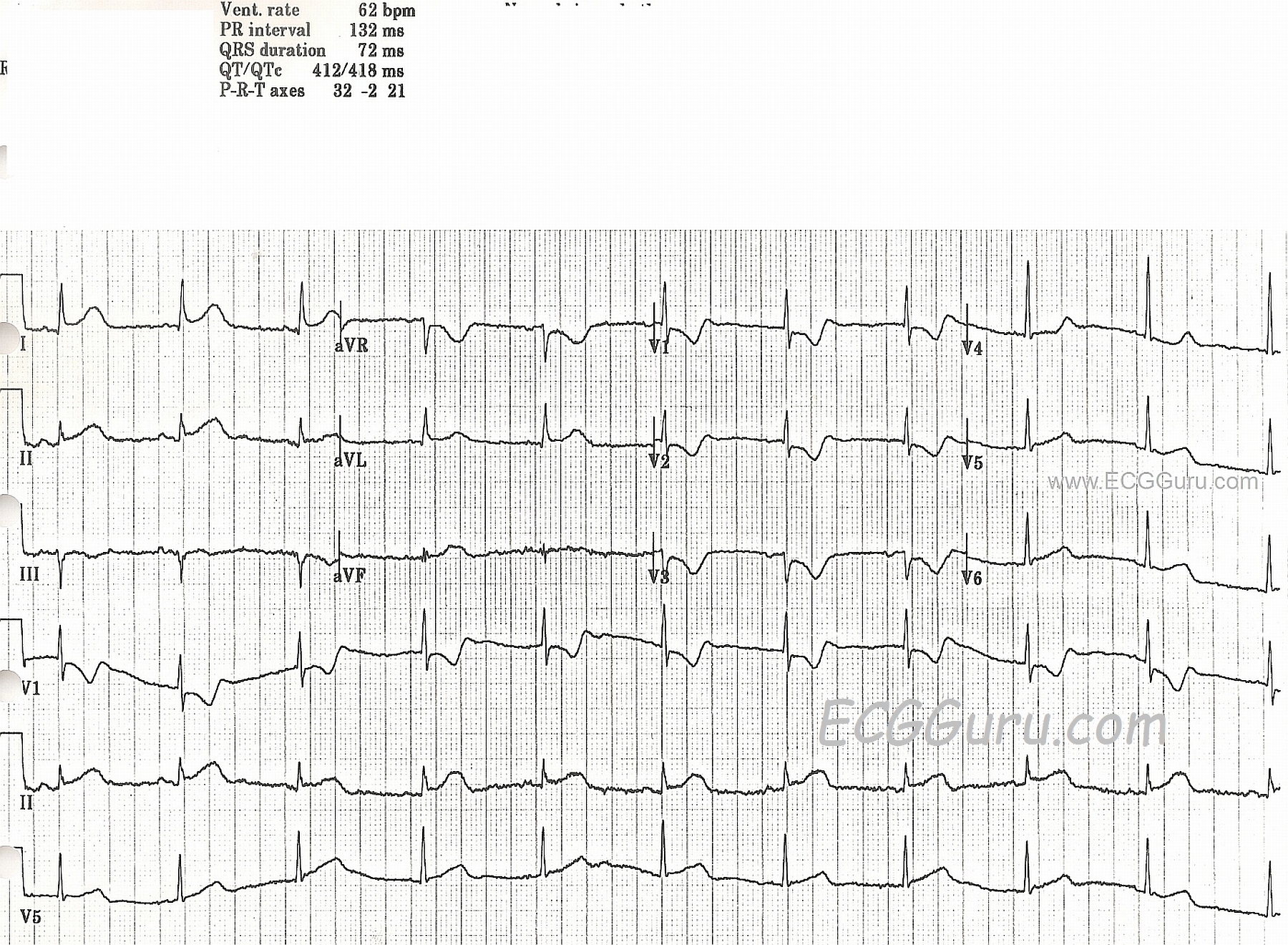
This ECG was obtained from a woman with chest pain who was taken to the cath lab and found to have a 100% occlusion of her circumflex artery.
There are obvious ST segment elevations in Leads I and aVL, as well as in Lead II. Lead II is the most leftward of the inferior wall leads, and I and aVL reflect the high lateral wall. She also has ST depressions in V1 through V3. If you look closely at the R wave progression in the anterior leads, you will readily note that it appears that V1 and V3 wires have been reversed. That being said, the "real" V2 and V3 have taller-than-normal R waves. The tall R waves and ST depression are signs of "posterior wall M.I." Recently, the actual definitions of the "lateral" wall and "posterior" wall have come into question. However, the important thing clinically, is that this patient IS experiencing an ST elevation M.I. (STEMI), which was confirmed in the cath lab. The locations of the ST changes were consistent with the 100% occlusion of her circumflex artery.
For our more advanced readers (and our "Gurus"), there is an interesting rhythm. The P wave morphology changes frequently, even though the rhythm remains regular. The rate, at 62 BPM, was adequate, and the patient did not suffer any consequential dysrhythmias during her procedure. We don't have long-term followup information on her.