This is a "classic" ECG of very good quality for you to use in a classroom setting.
The Patient: A 57-year-old man who complains of a sudden onset of "sharp" chest pain while on a long bike ride. The pain does not radiate, and nothing makes it worse or better. He is pale, cool, and diaphoretic. His medical history is unknown.
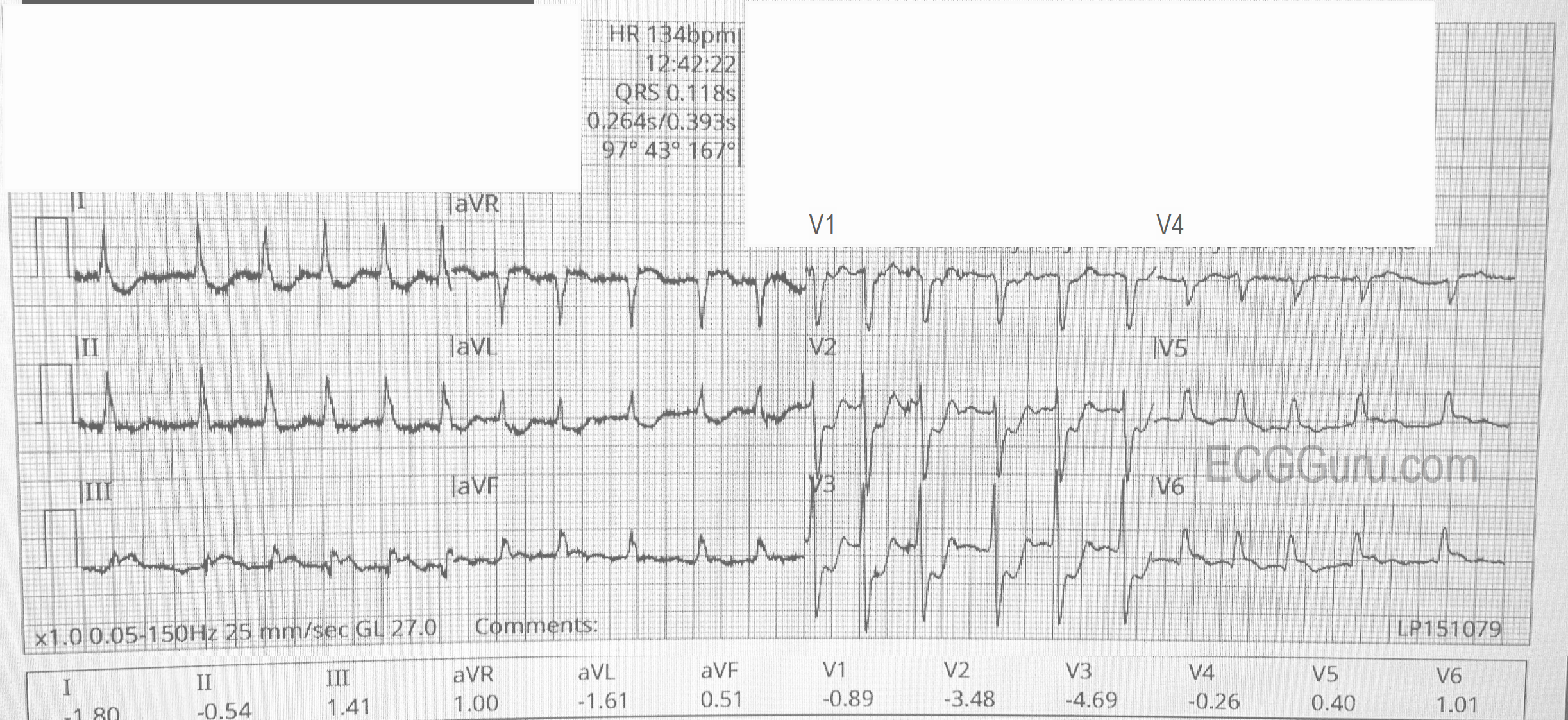
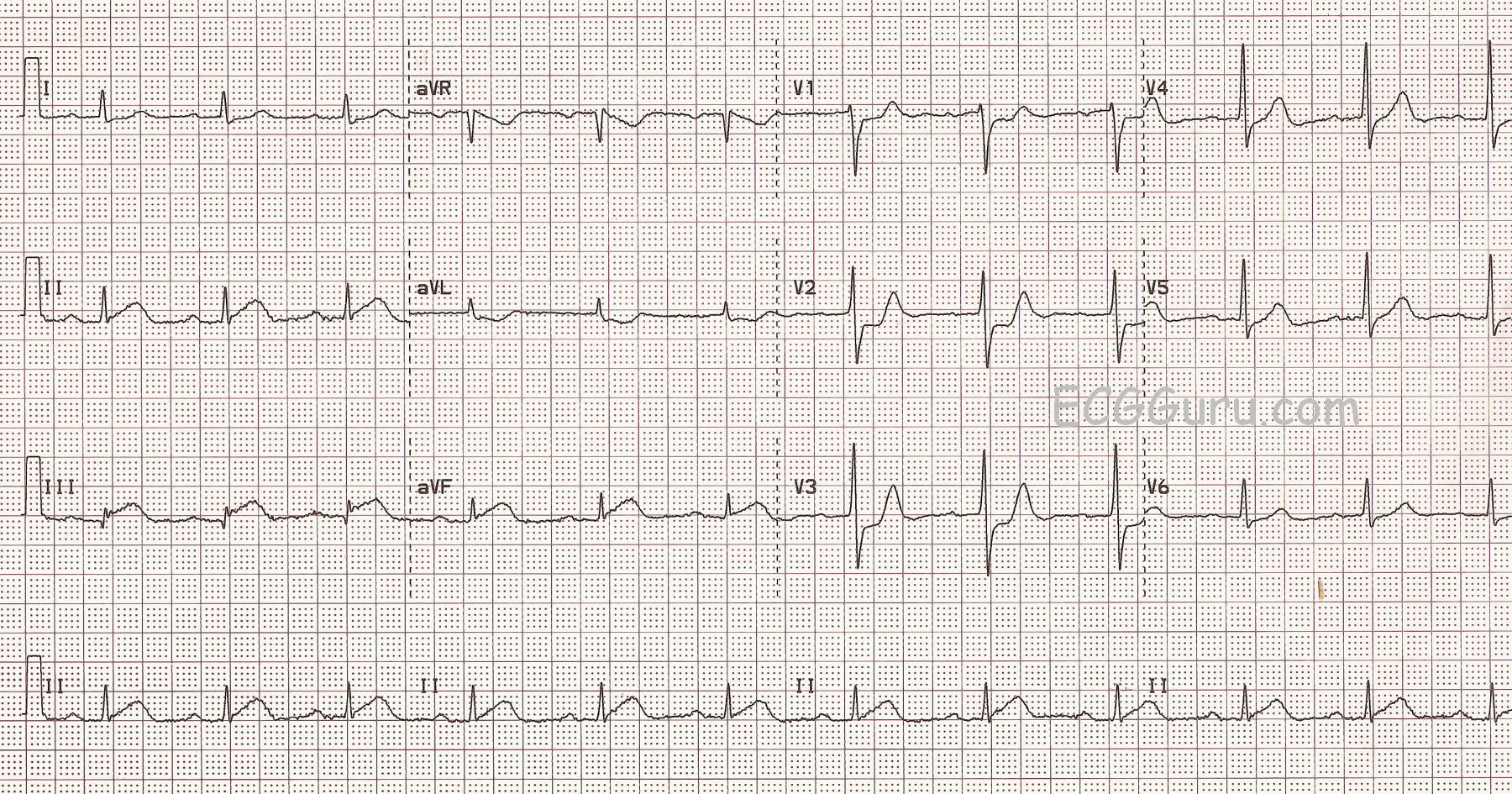
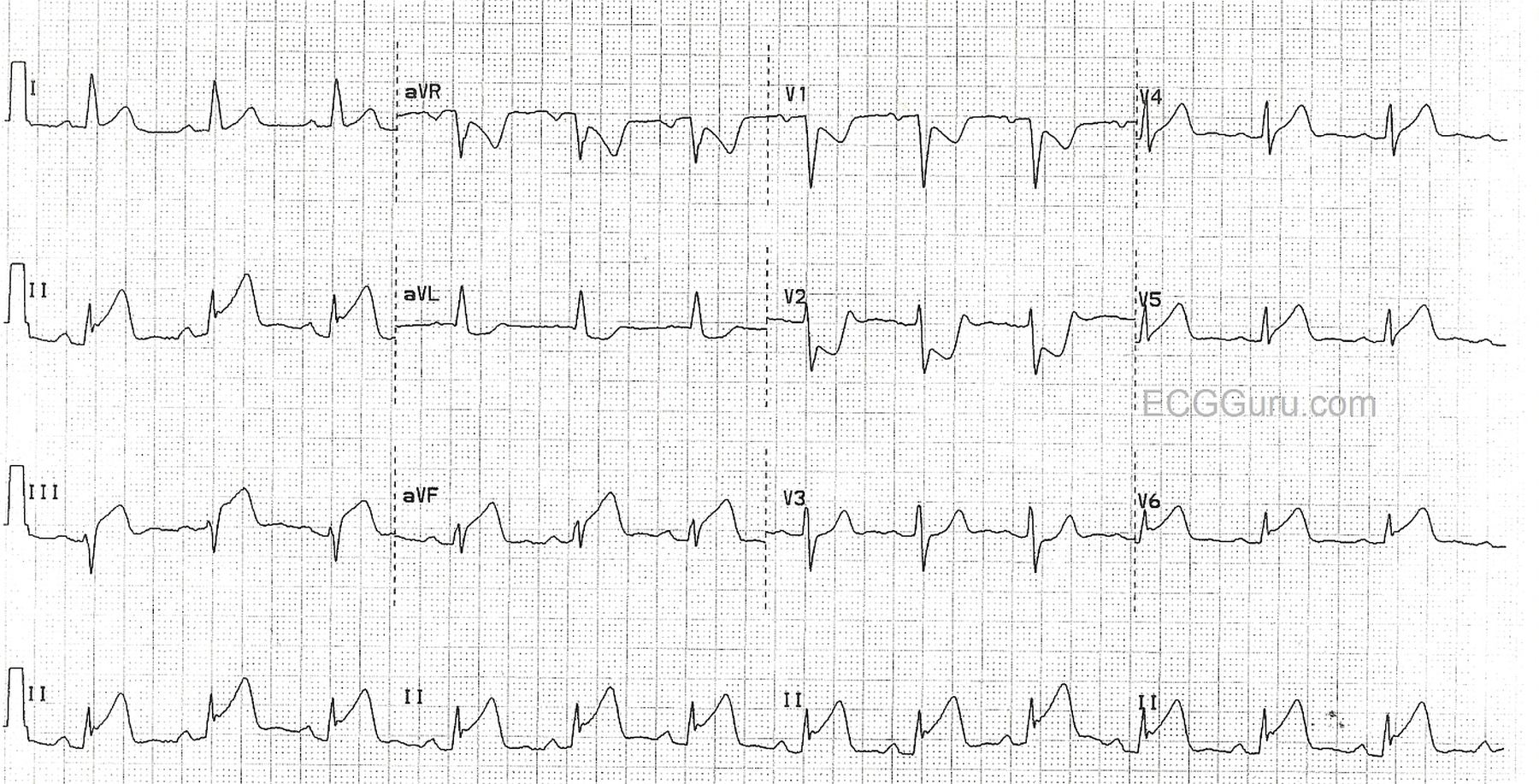
The ECG: This ECG could be considered "classic" for an inferior wall ST elevation M.I. caused by occlusion of the right coronary artery. ECG findings include:
* Normal sinus rhythm
* Marked ST elevation in Leads II, III, and aVF. The elevation is higher in Lead III than in Lead II, a reliable sign of RCA occlusion.
* Reciprocal depression in Leads aVL and I. ST depression in the setting of acute transmural ischemia (STEMI) is almost ALWAYS due to reciprocal change. The fact that this STD is localized to leads that are reciprocal to the inferior wall is proof of the nature of the STD.
* Reciprocal depression in V1 - V3. More localized depression. What wall is reciprocal to the anterior-septal wall? The posterior (postero-lateral). Since the inferior wall is really the lower part of the posterior wall, inferior wall M.I. is often accompanied by posterior wall M.I.
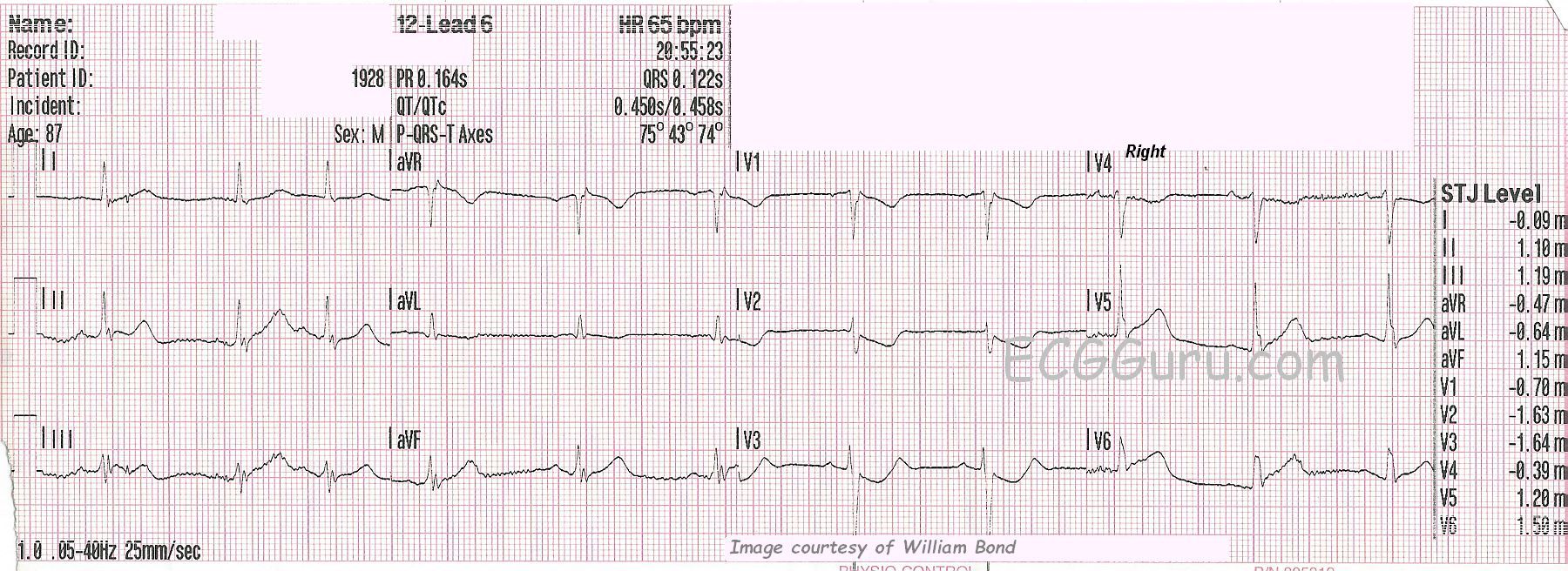
An additional lead, V4R, is helpful in this situation, since the right ventricle is often affected in RCA occlusions. The EMS crew reports that V4R was negative for ST elevation, but we do not have a copy.
Small q waves have formed in Lead III, and we would watch for progression of this sign, as it can indicate necrosis.
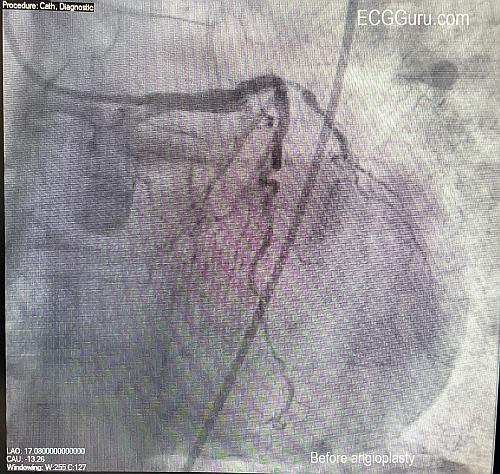
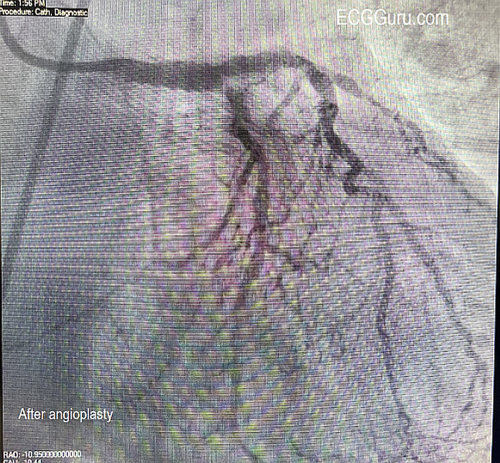
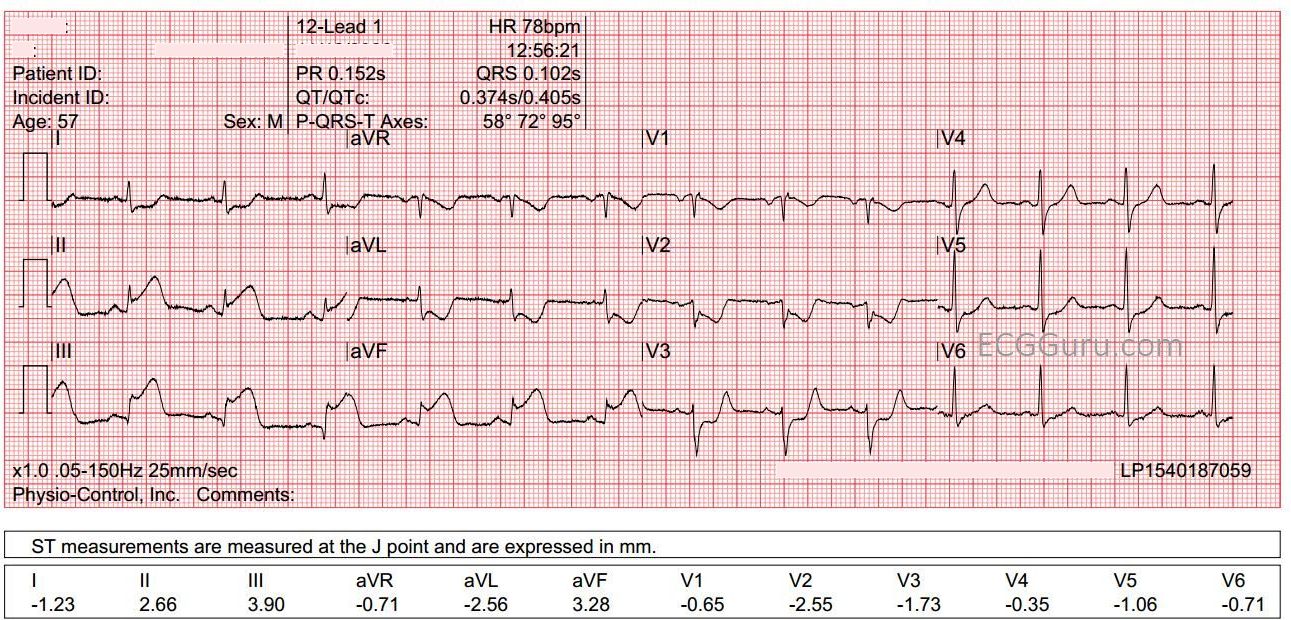
Outcome: The patient went to the cath lab, but we have no further followup.
Our thanks to Ashley Terrana for donating this tracing.