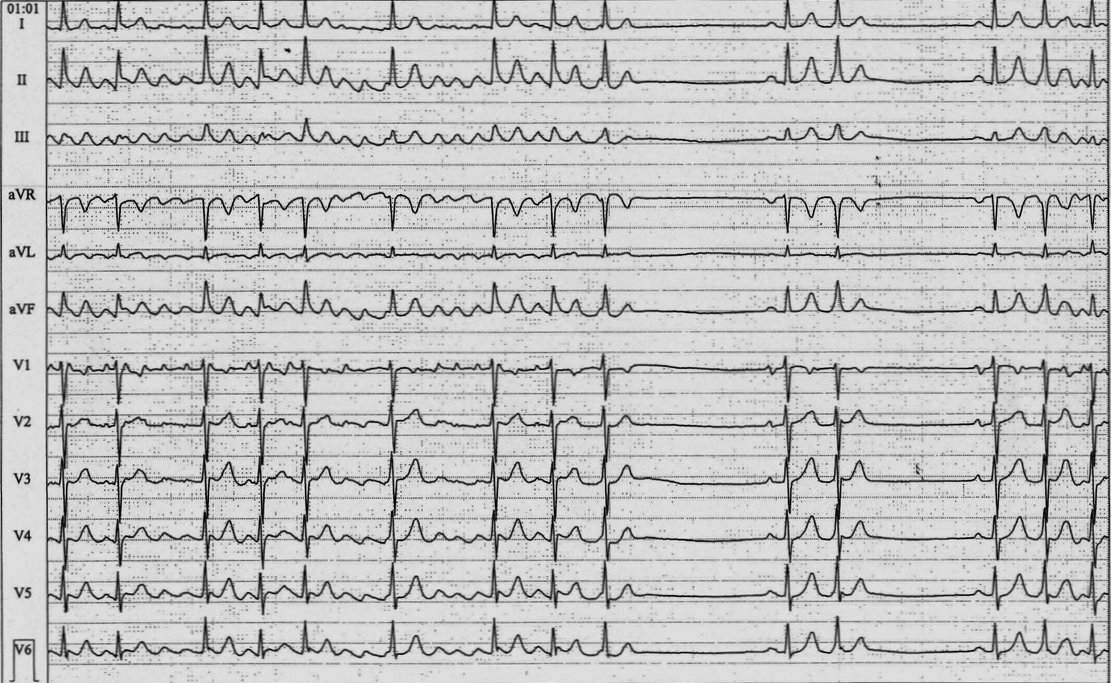
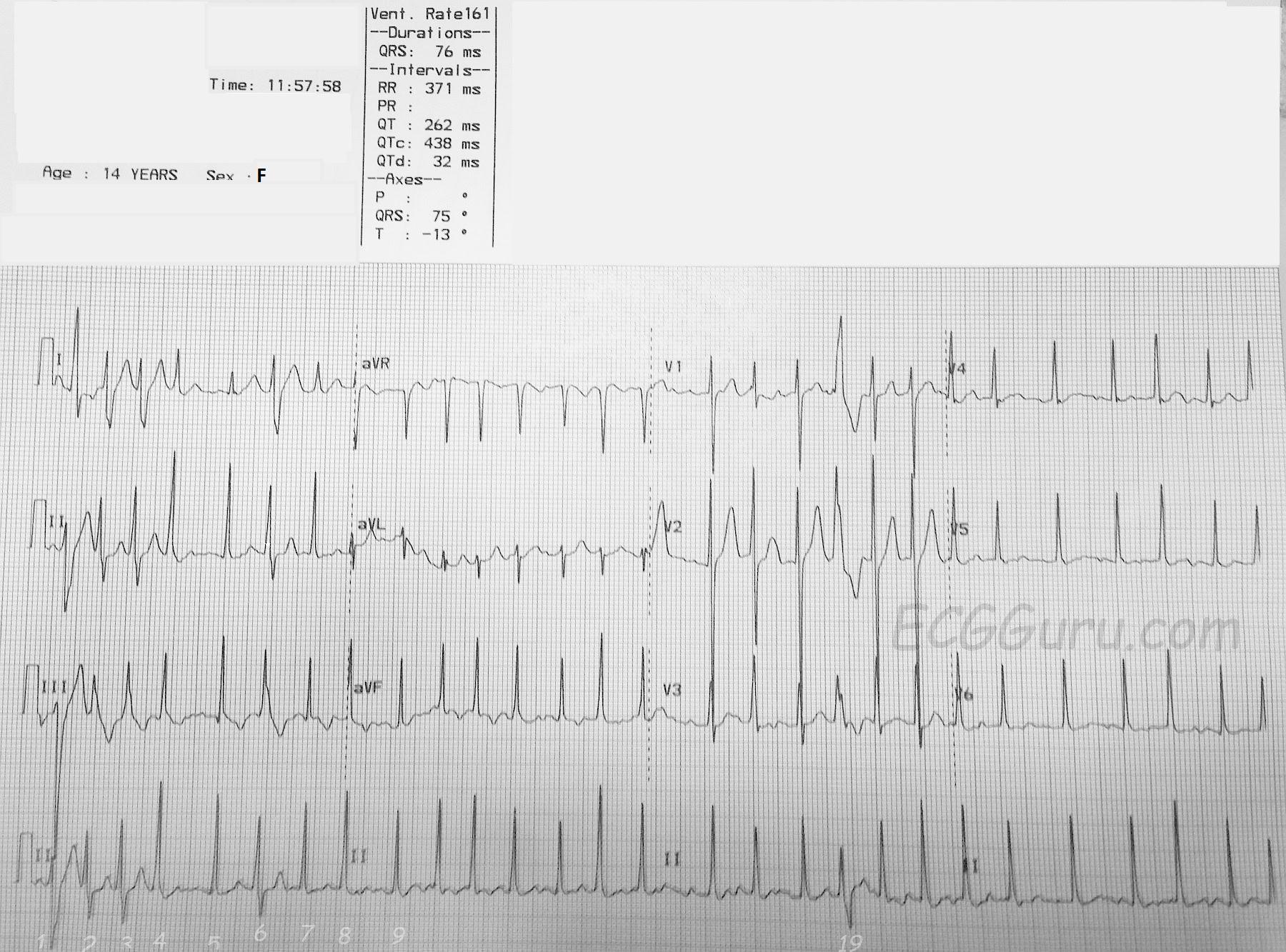
The Patient: This ECG was taken from a 14-year-old girl with a complaint of palpitations. Her medical history is not known.
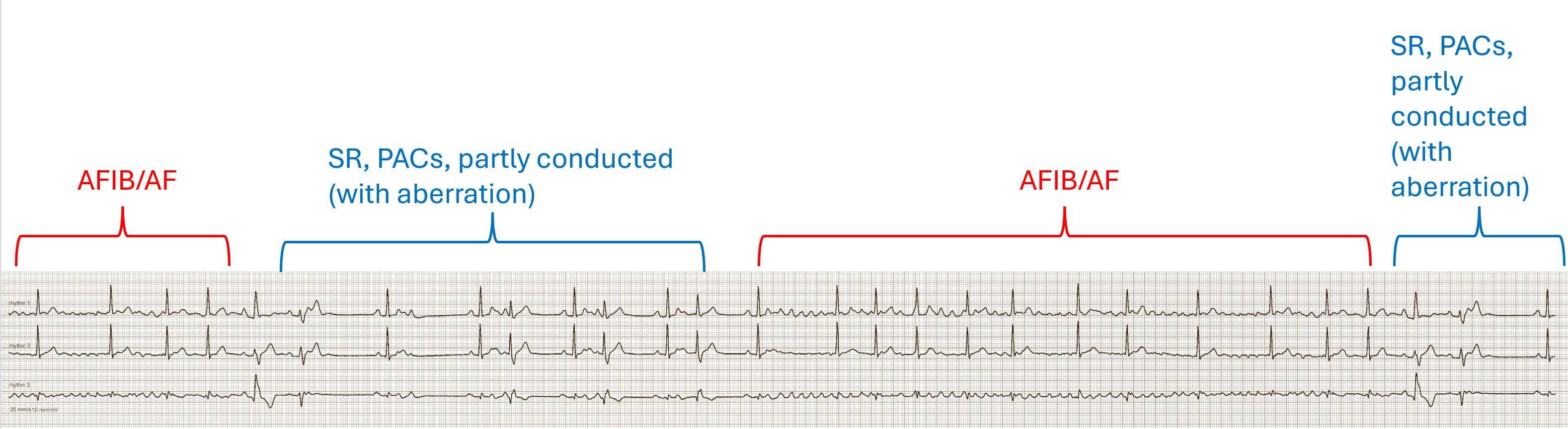
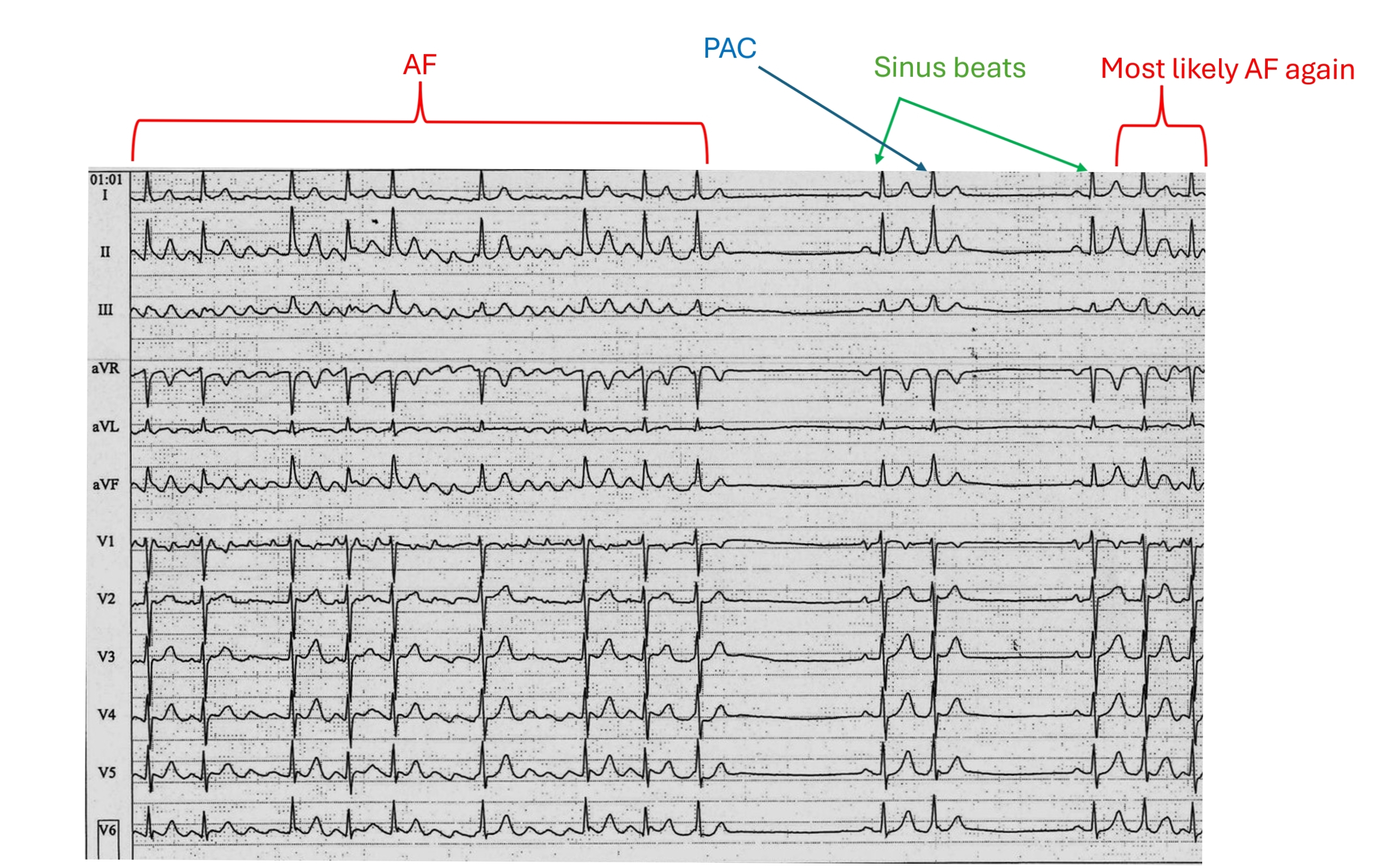
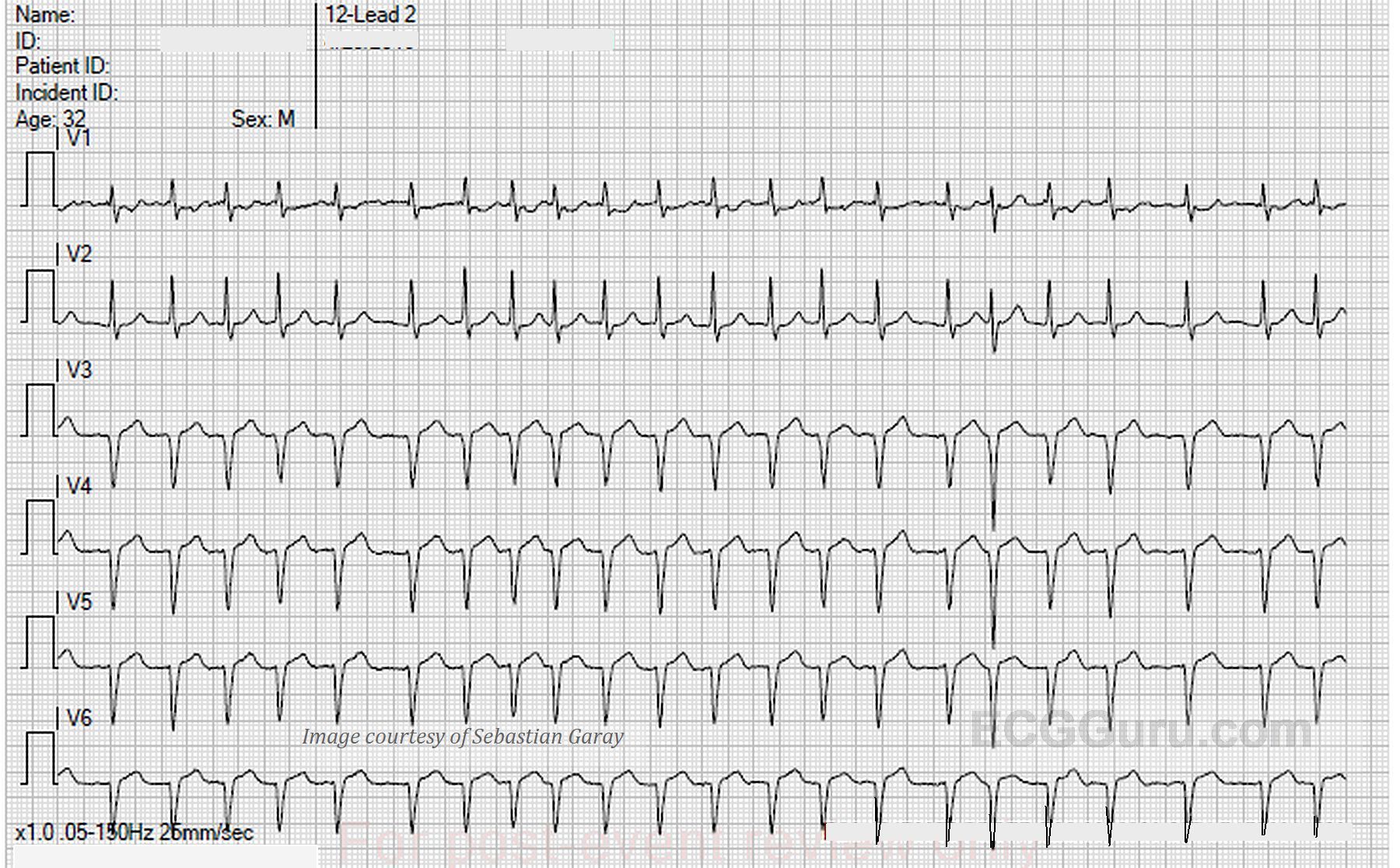
The ECG: The rate is about 160 bpm, with an irregularly-irregular rhythm. There are no P waves. This is atrial fibrillation. There are several different morphologies noted in the QRS complexes. First, a narrow QRS with normal axis, as demonstrated in beats #5 and #7. There are distinctly wide QRS complexes with a right bundle branch block pattern. See beats #2, #3, and #19. This represents aberrant conduction. Atrial fib often displays aberrant conduction, especially when a beat follows closely after a long R-R cycle followed by a short R-R cycle. The refractory period is set by the preceding cycle. So a lont R-R causes a longer refractory period. The short R-R that follows finds itself in a relative refractory period - not refractory enough to prevent conduction altogether, but in this case, the right bundle branch has not yet recovered, so the impulse continues down the left bundle, bypassing the right bundle branch. The right ventricle depolarizes late, causing a widening of the QRS.
There is a sliight variation seen in the aberrant beats, notably in #1 and #2. This may represent varying amounts of aberrancy, where the pathways change slightly from beat to beat. Atrial fibrillation is rare in children and adolescents, but can be caused by many factors, including stress, caffeine, endocrine disorders, obesity, and heart infections.
This ECG was published by me on Facebook nearly a decade ago, and received some excellent comments from Dave Richley and Dr. Ken Grauer (two of our favorite Gurus). I will reproduce them here to spare them re-writing their comments.