
Submitted by Dawn on Tue, 05/23/2023 - 15:59
The Patient: This ECG was taken from a 14-year-old girl with a complaint of palpitations. Her medical history is not known.
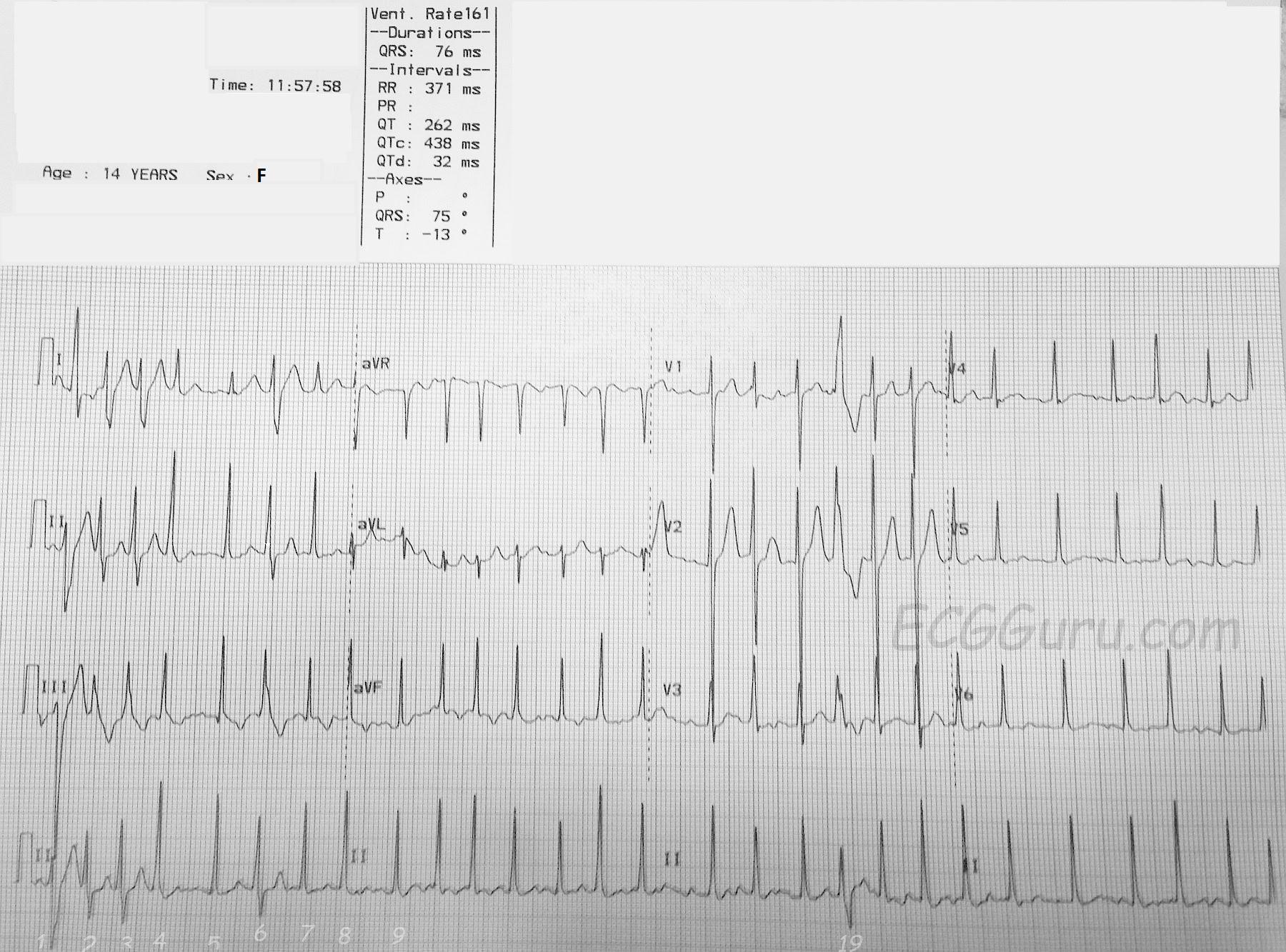
The ECG: The rate is about 160 bpm, with an irregularly-irregular rhythm. There are no P waves. This is atrial fibrillation. There are several different morphologies noted in the QRS complexes. First, a narrow QRS with normal axis, as demonstrated in beats #5 and #7. There are distinctly wide QRS complexes with a right bundle branch block pattern. See beats #2, #3, and #19. This represents aberrant conduction. Atrial fib often displays aberrant conduction, especially when a beat follows closely after a long R-R cycle followed by a short R-R cycle. The refractory period is set by the preceding cycle. So a lont R-R causes a longer refractory period. The short R-R that follows finds itself in a relative refractory period - not refractory enough to prevent conduction altogether, but in this case, the right bundle branch has not yet recovered, so the impulse continues down the left bundle, bypassing the right bundle branch. The right ventricle depolarizes late, causing a widening of the QRS.
There is a sliight variation seen in the aberrant beats, notably in #1 and #2. This may represent varying amounts of aberrancy, where the pathways change slightly from beat to beat. Atrial fibrillation is rare in children and adolescents, but can be caused by many factors, including stress, caffeine, endocrine disorders, obesity, and heart infections.
This ECG was published by me on Facebook nearly a decade ago, and received some excellent comments from Dave Richley and Dr. Ken Grauer (two of our favorite Gurus). I will reproduce them here to spare them re-writing their comments.
This is atrial fibrillation and I think that the beats labelled 1, 2, 3, 6 and 19 all show aberrant conduction (to various degrees). These beats may well be examples of the Ashman phenomenon in which the aberrancy follows a long RR-short RR sequence, but we would need to see a longer strip to be sure. Beat 1 appears to be conducted with a RBBB/LAFB pattern, whereas the other broad QRS complexes appear to show just a RBBB pattern (although LPFB in addition is a possibility). There is continuous variation in R-wave height through the lead II rhythm strip. This may be related to varying degrees of aberrancy, but perhaps it’s more likely to be at least partly due to respiratory chest wall movement because the variation appears to follow a regular ‘waxing and waning’ pattern.
Agree - rapid AFib with probably all aberrant conduction. The very first beat seems to have LAHB in addition to RBBB aberration - beats #2,3 don't have the LAHB ...
I don't think this an optimal illustration of Ashman phenomenon (Dave could have guessed I'd say that ....). Why doesn't the 2nd complex in V1 show more aberration than the 4th complex in V1? Now I know that the coupling interval of this 2nd beat in V1 is indeed slightly longer than the coupling interval of the 4th beat in V1 - but the preceding R-R before this 2nd beat is much longer than the preceding R-R of the 4th beat, so if true "Ashman" - I would have expected a greater degree of aberration for this 2nd beat. Otherwise - all we have is a relative long-short for the 6th complex in the long lead II with no information on preceding R-R intervals before the first 3 aberrant beats. Bottom Line - To invoke Ashman here I think is stretching it .... but I realize others may see the above in different light. That said - at least we can all agree this is rapid AFib with expected aberrant conduction
Follow Up: The patient was diagnosed in the ER with "Atrial Flutter" and successfully cardioverted. We do not know the cause of the dysrhythmia or the outcome of the case. Our thanks to Ryan Cihowiak RN, Paramedic, for donating this interesting case.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Very Thought-Provoking Tracing
I tend to agree with Ken that the aberrancy is likely not due to the Ashman phenomenon. Good examples of the Ashman phenomenon during atrial fibrillation that I have seen have been tracings with more controlled (i.e., slower) rates. In this ECG, I think the aberrant conduction is due to those impulses getting through the AV node in such great numbers that they are finding the ventricles in various states of irregular refractoriness.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd