The Patient: This ECG and rhythm strip are from a man in his early sixties. He was in his cardiologist’s office, complaining of a very rapid heart rate and weakness for several hours. He was standing, and denied pain, shortness of breath, or dizziness. The vital signs were not shared with us, but the patient was warm and dry, alert and oriented, and ambulatory. We are told that he has an unspecified myopathy and an automatic implanted cardioverter/defibrillator (AICD).
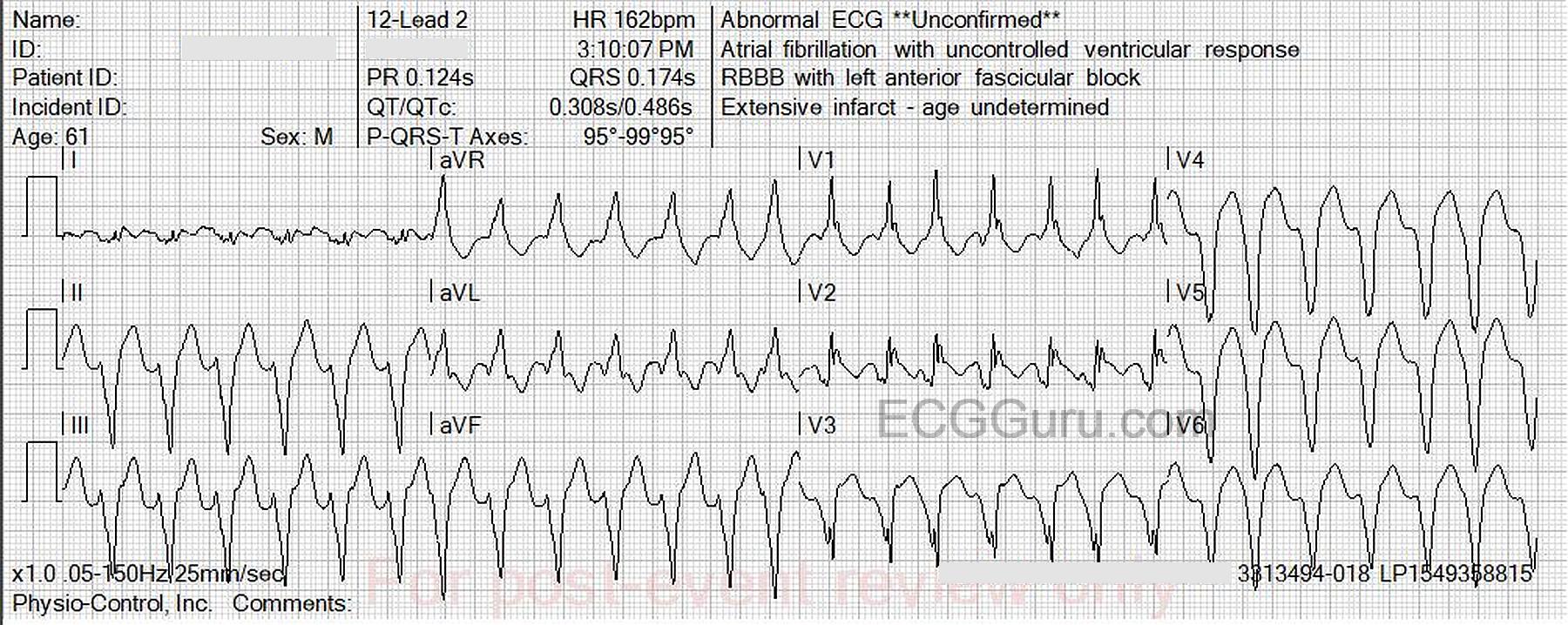
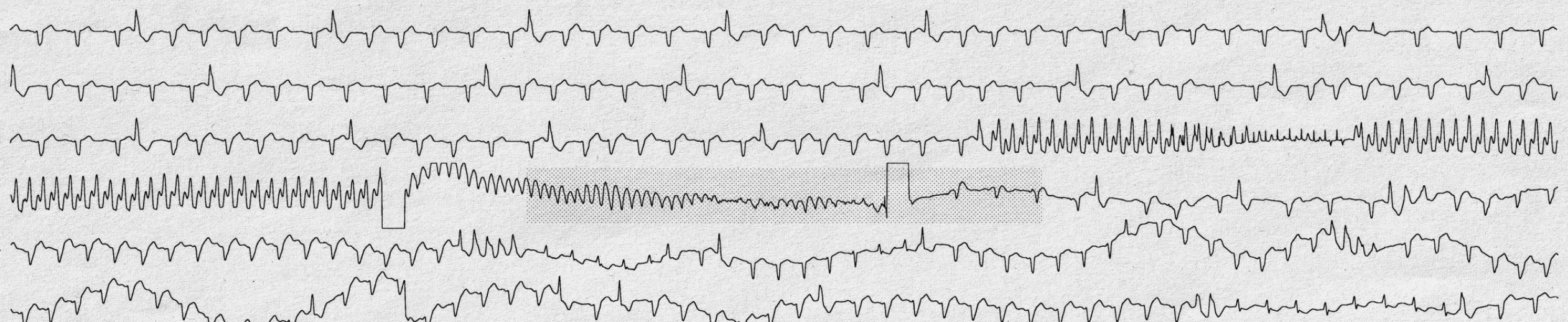
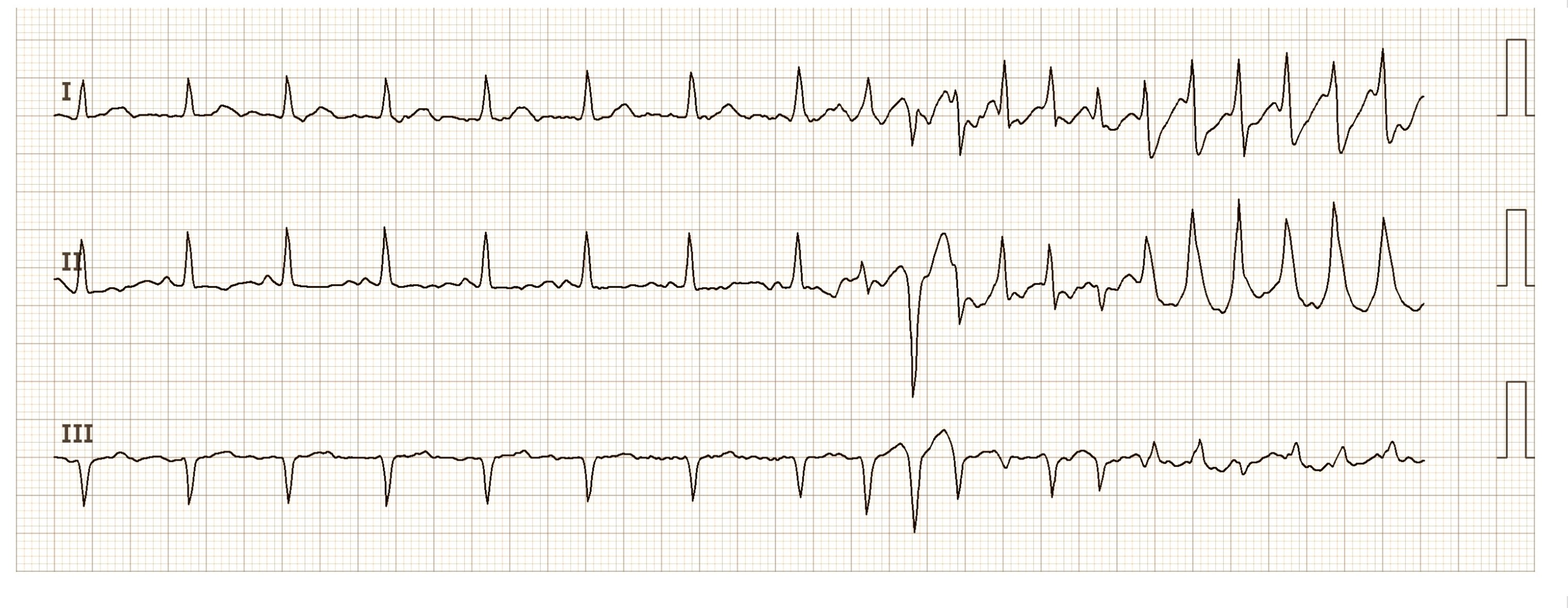
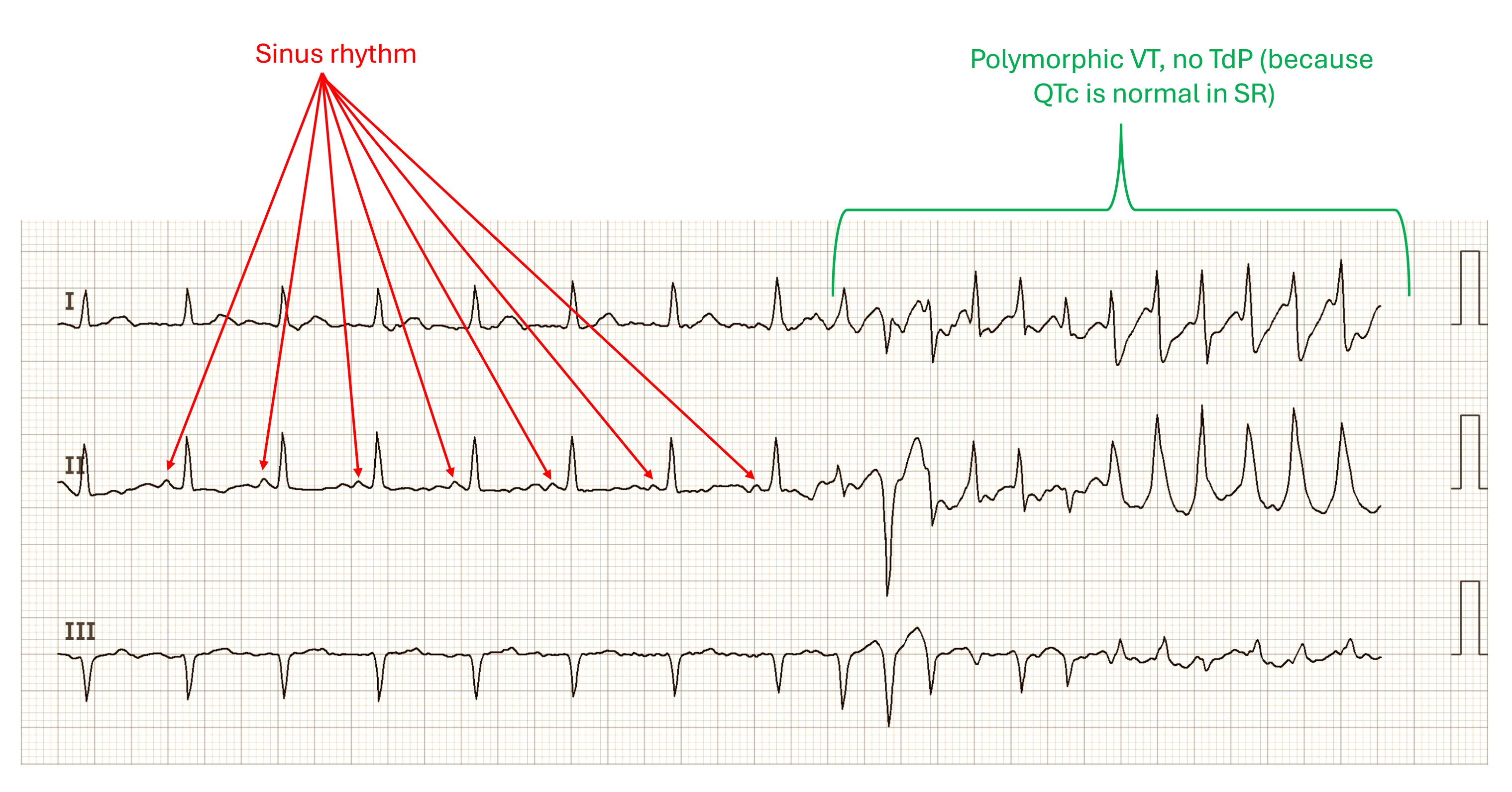
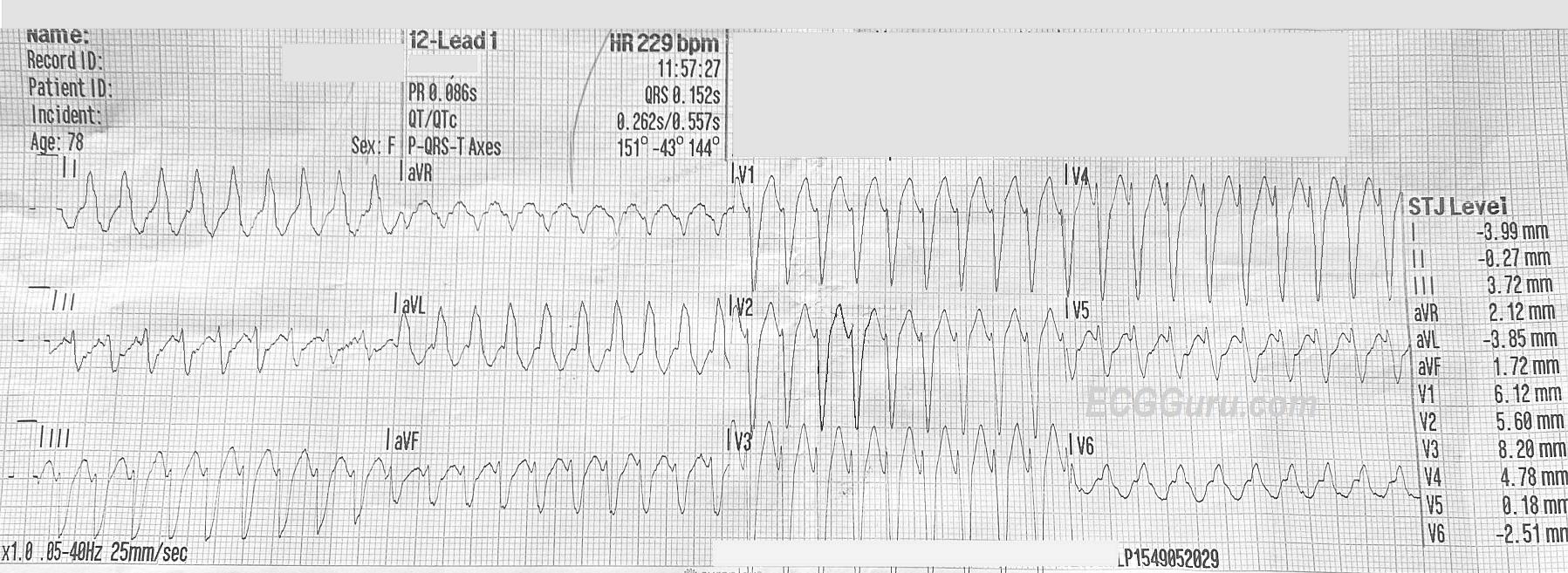
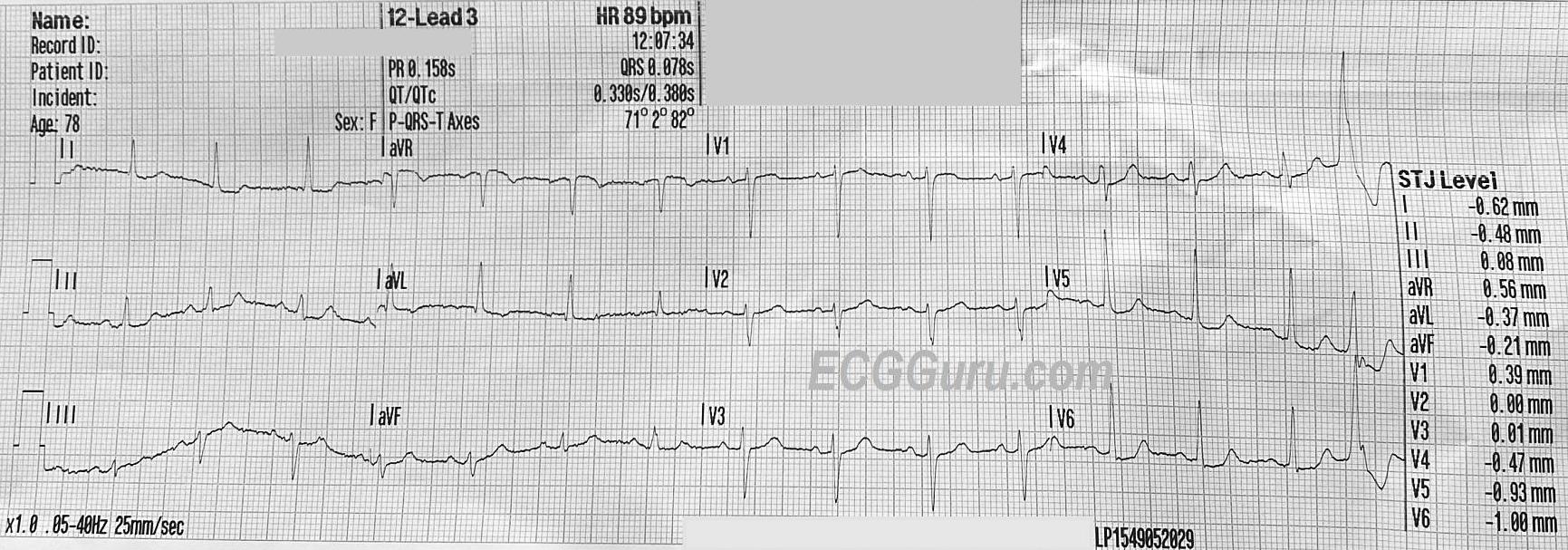
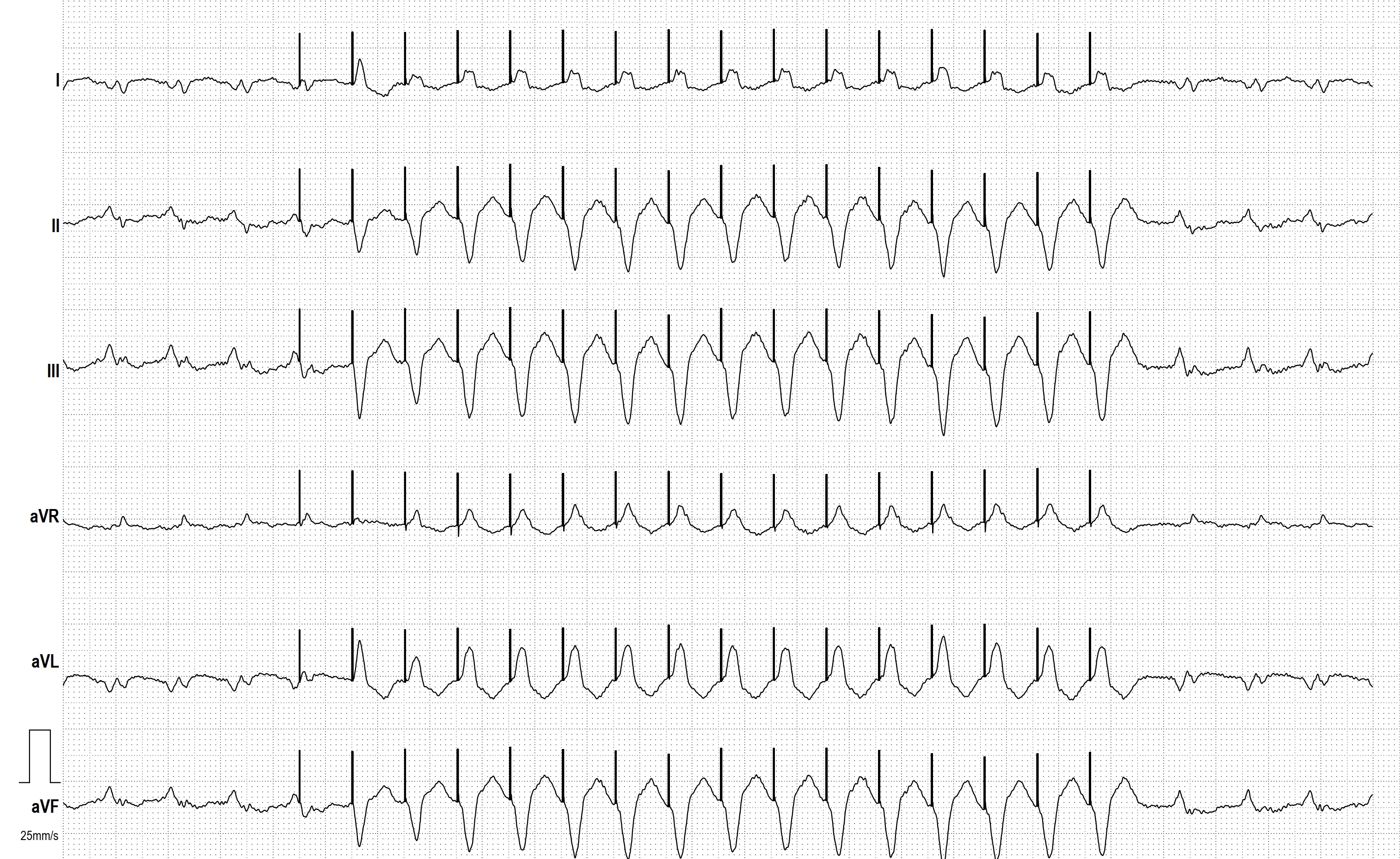
The 12-Lead ECG: There is a wide complex (0.174 sec.) tachycardia (WCT) at 162 bpm. The rhythm is slightly irregular, triggering an interpretation of “atrial fibrillation” by the machine. The computer also suggested right bundle branch block and anterior fascicular block (bifascicular block). I do not agree with this. I see a WCT that does not have the typical QRS pattern of RBBB or bifascicular block. There is an underlying REGULAR rhythm, with occasional premature beats that resemble, but are not identical to, the regular beats. (See rhythm strip included).
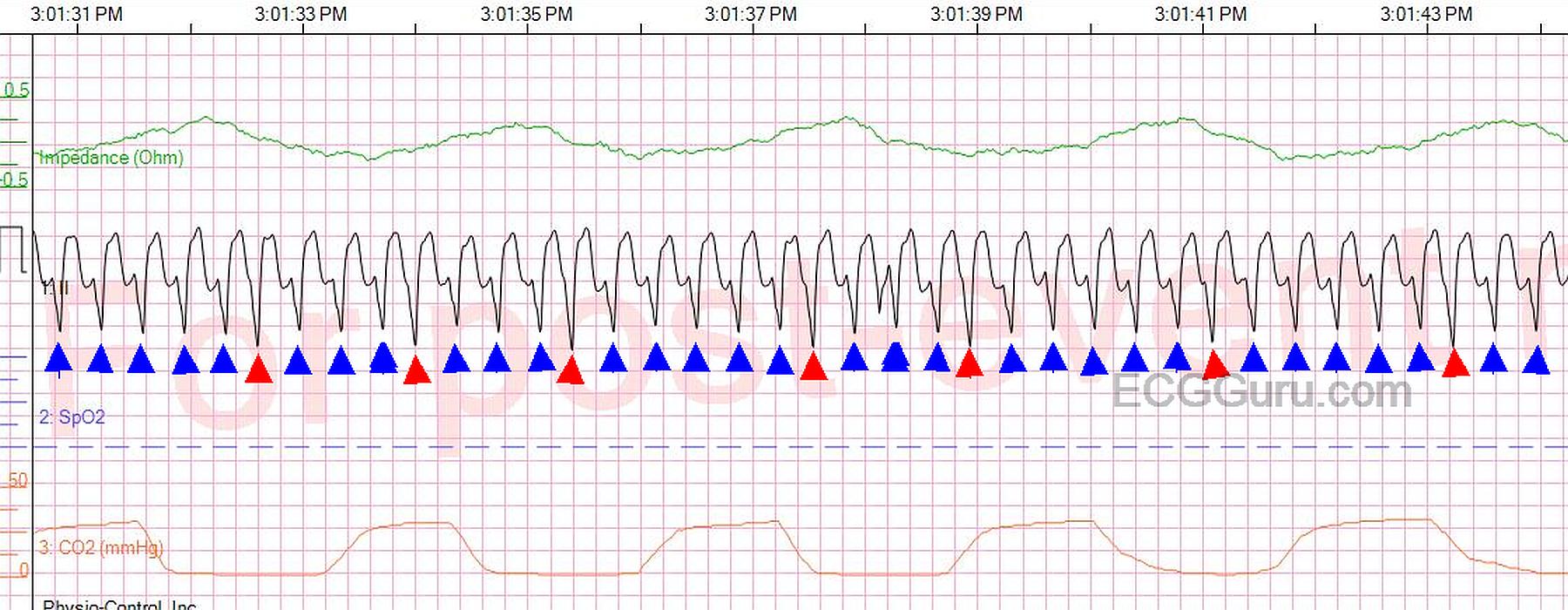
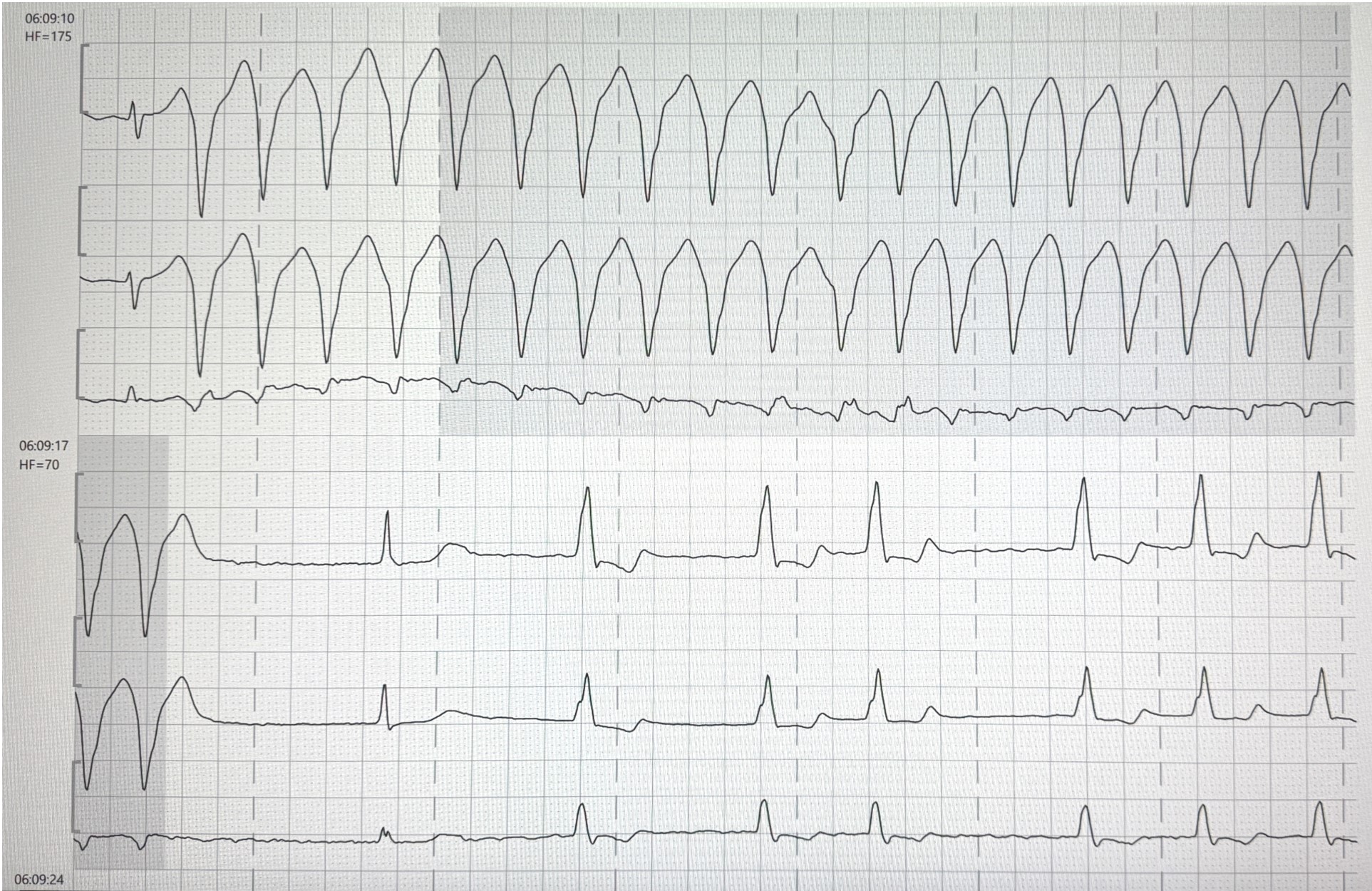
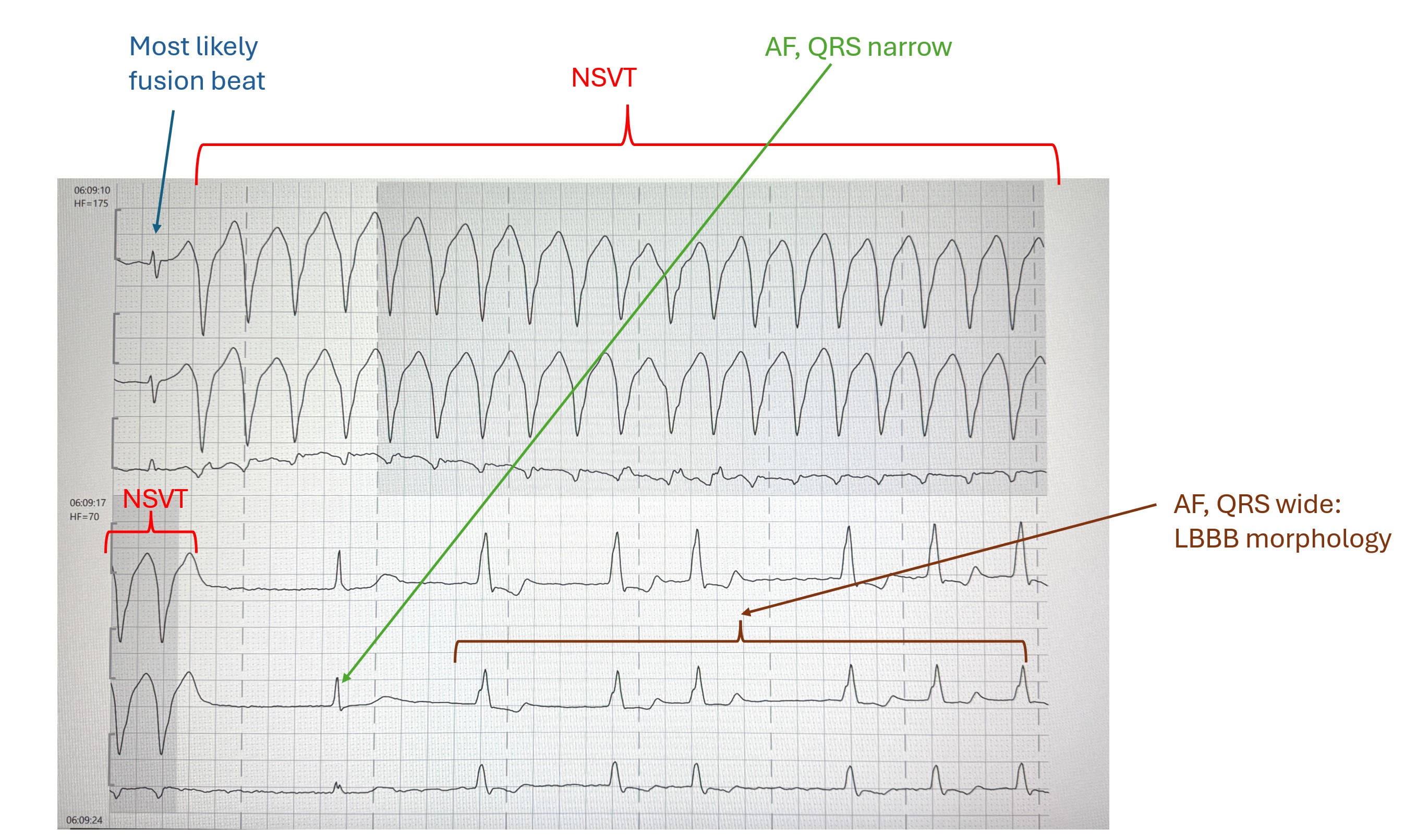
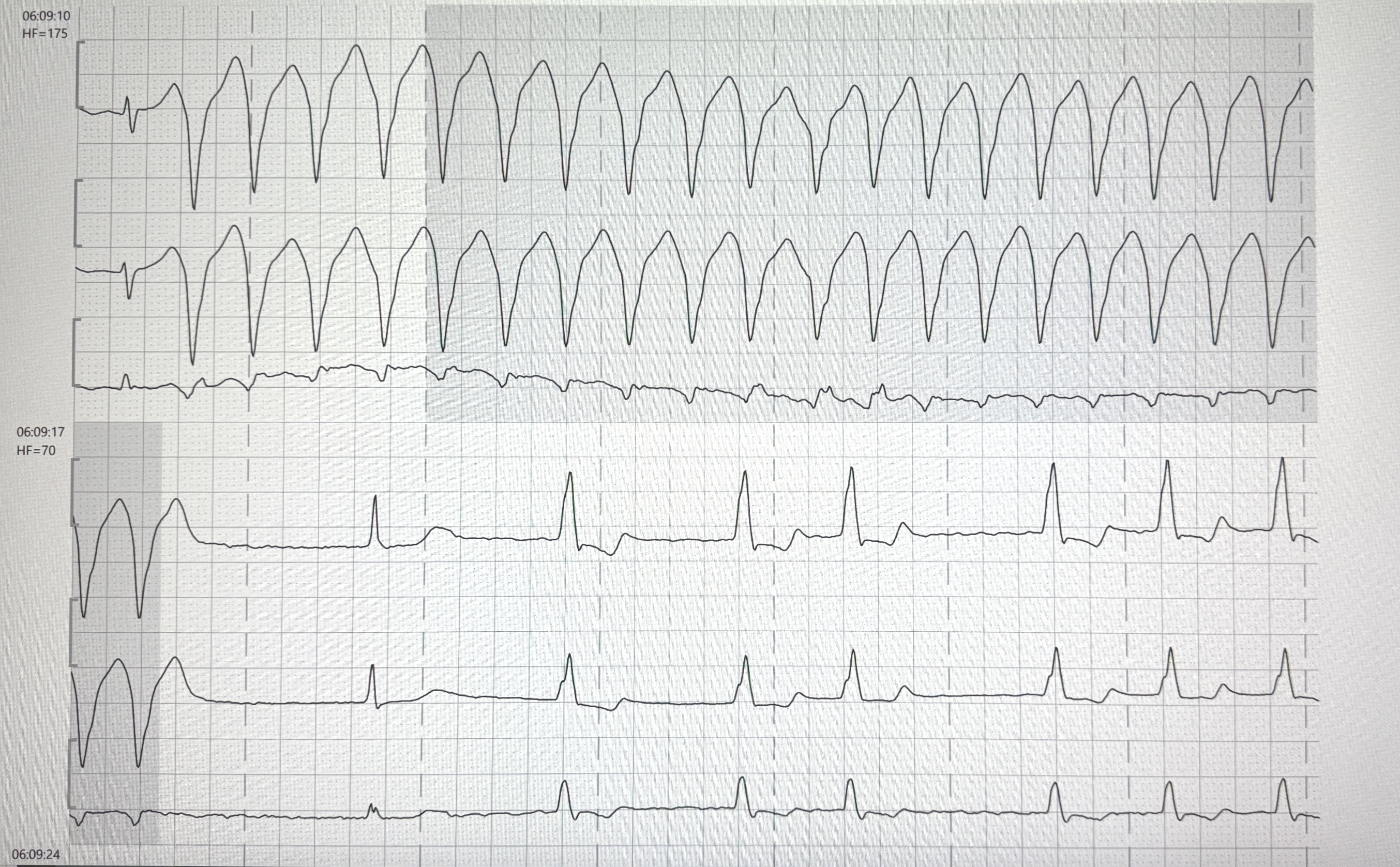
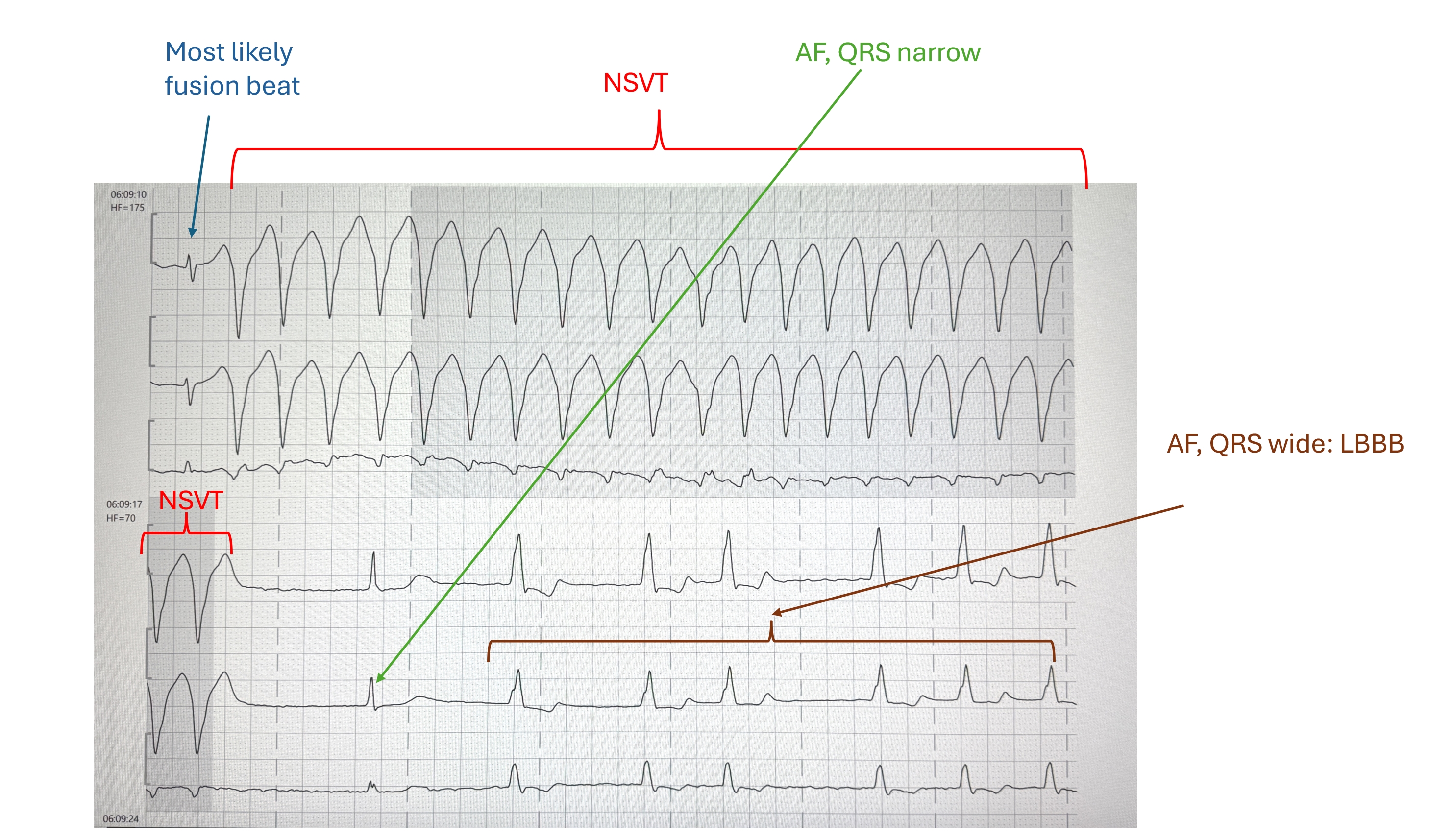
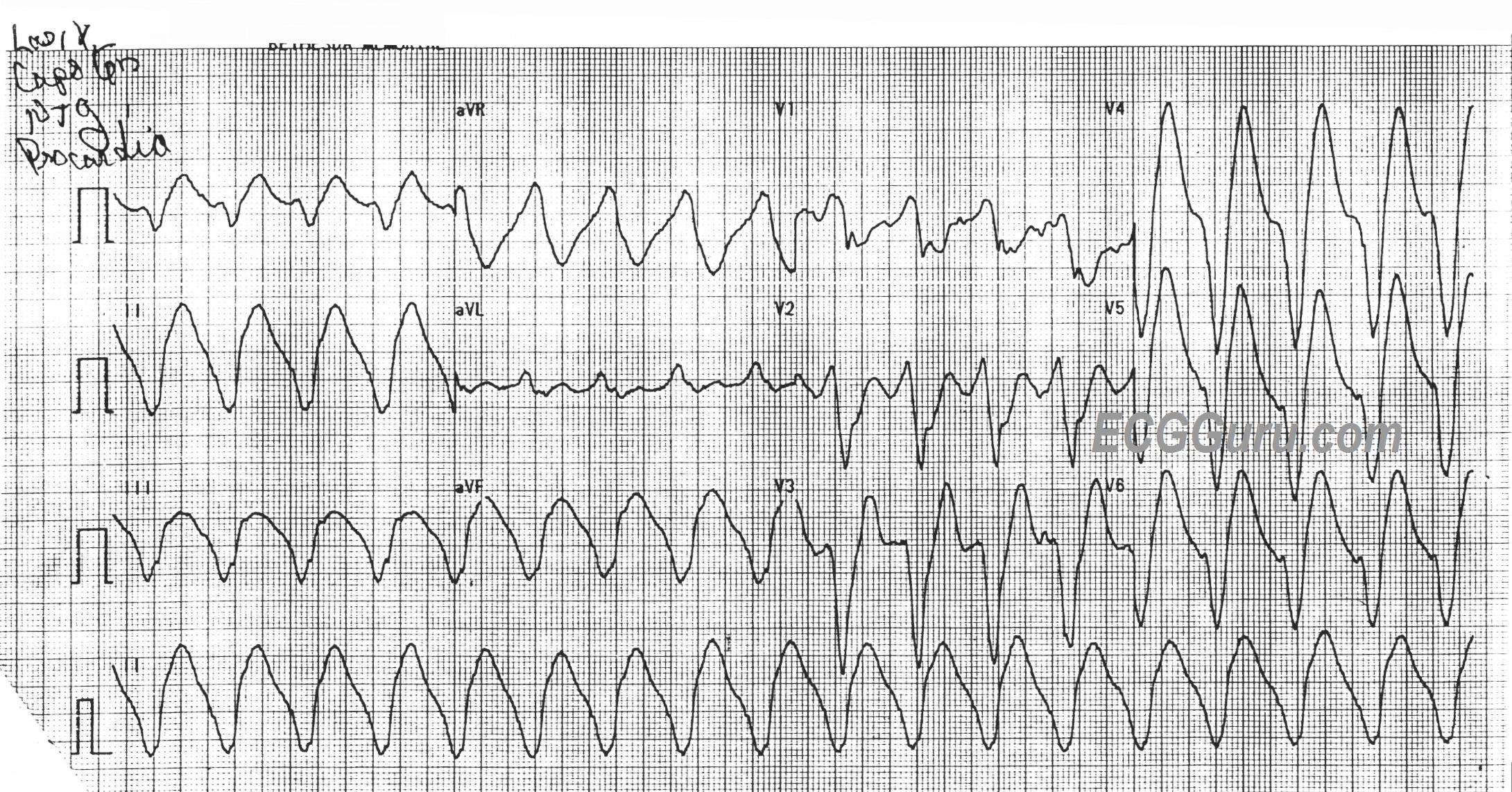
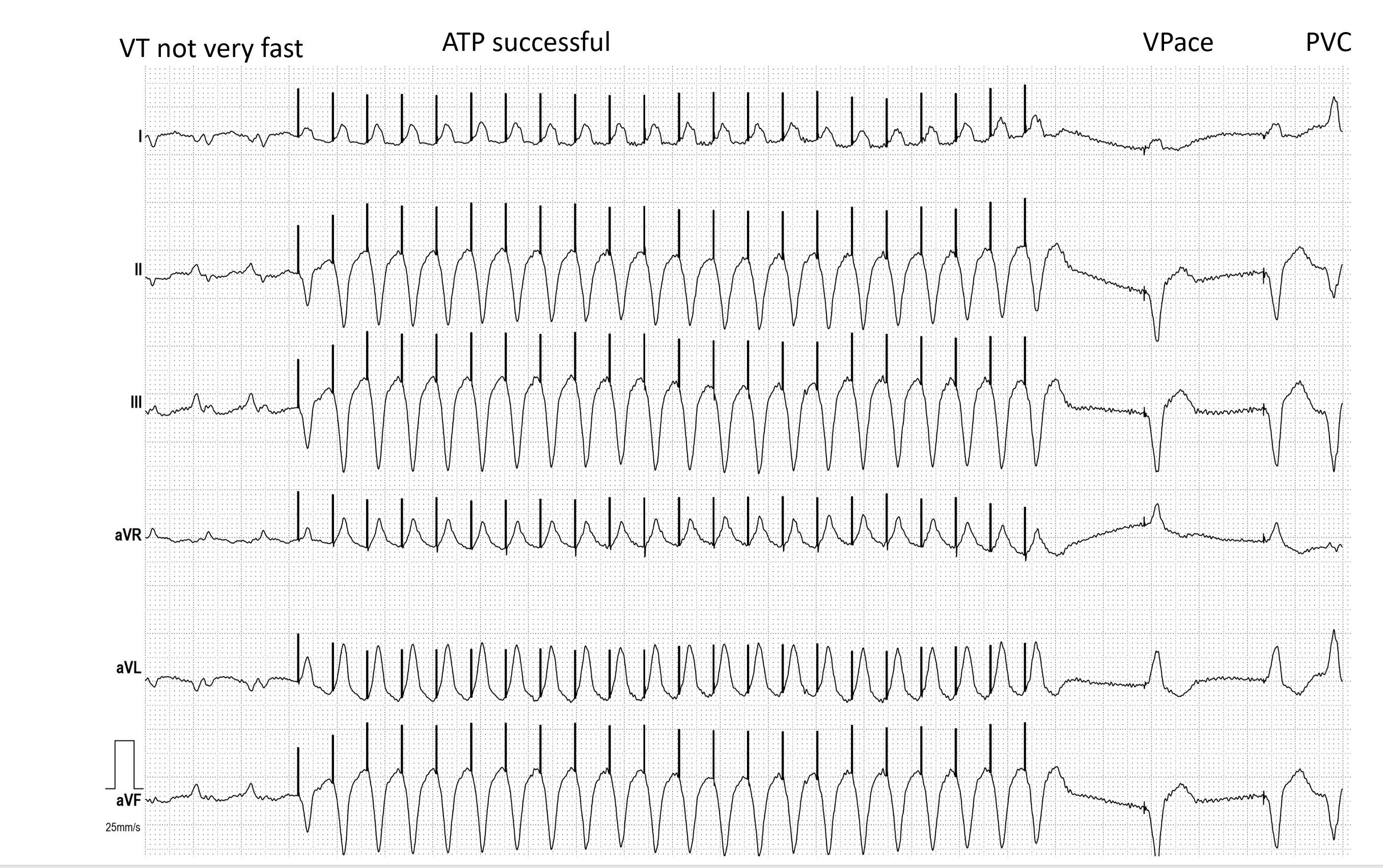
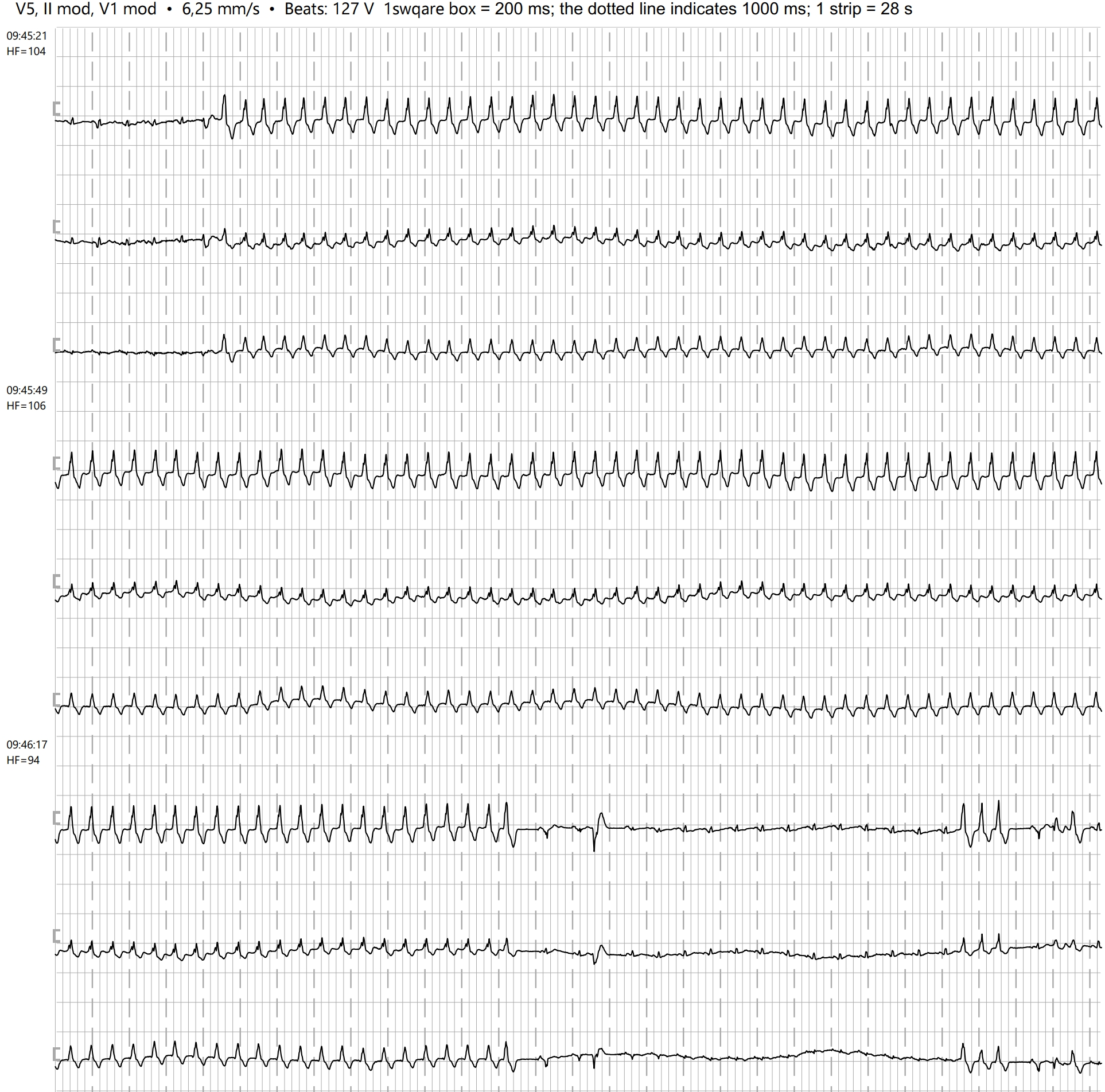
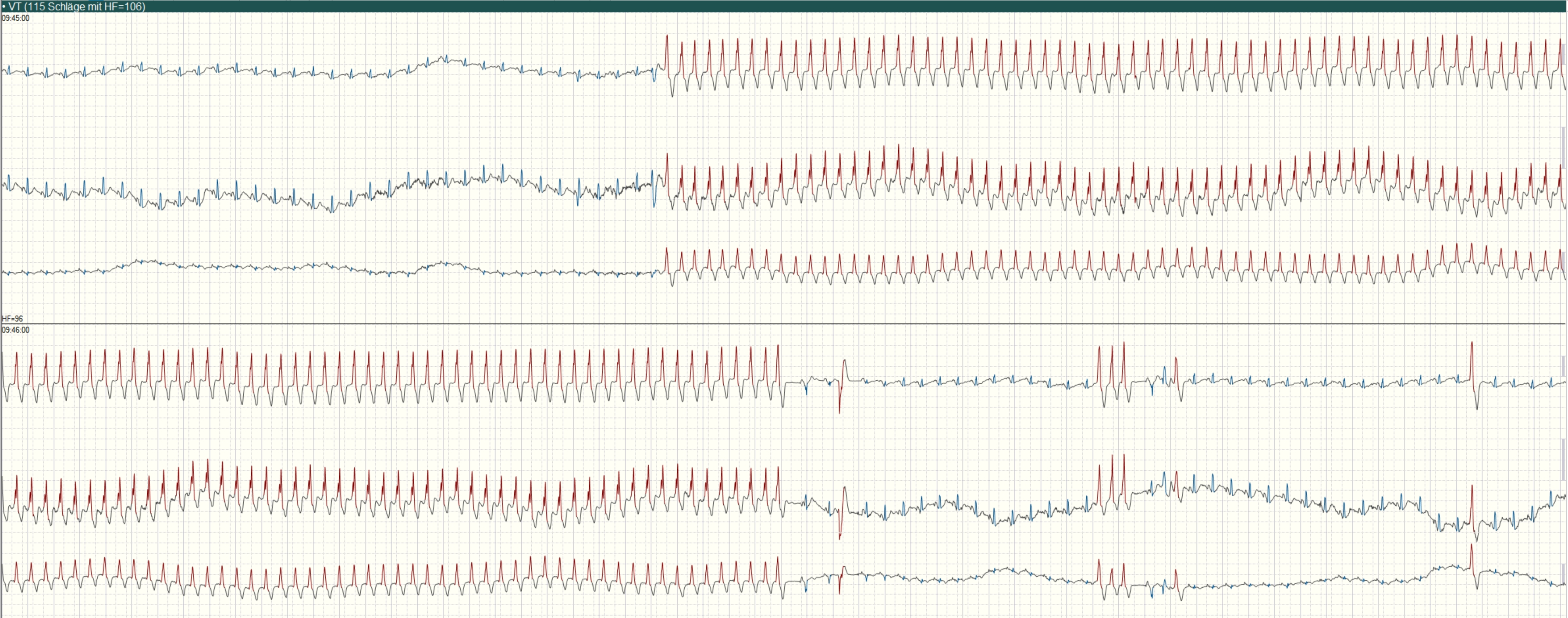
This rhythm is V Tach. Often, especially in an emergency setting, V Tach is a re-entrant tachycardia, characterized by a sudden onset and offset and a fast, regular rhythm. In this case, the V Tach is interrupted every 3-5 beats by a PVC. This tells us that the V Tach is due to increased automaticity or triggered activity, as a PVC would abolish the re-entry cycle. The PVCs look very similar to the “regular” V Tach beats, but are not exactly the same. So, the PVCs are coming from a focus very near the origin of the V Tach. This regular rhythm with frequent PVCs is easier to appreciate on the long rhythm strip provided, which rules out atrial fibrillation.