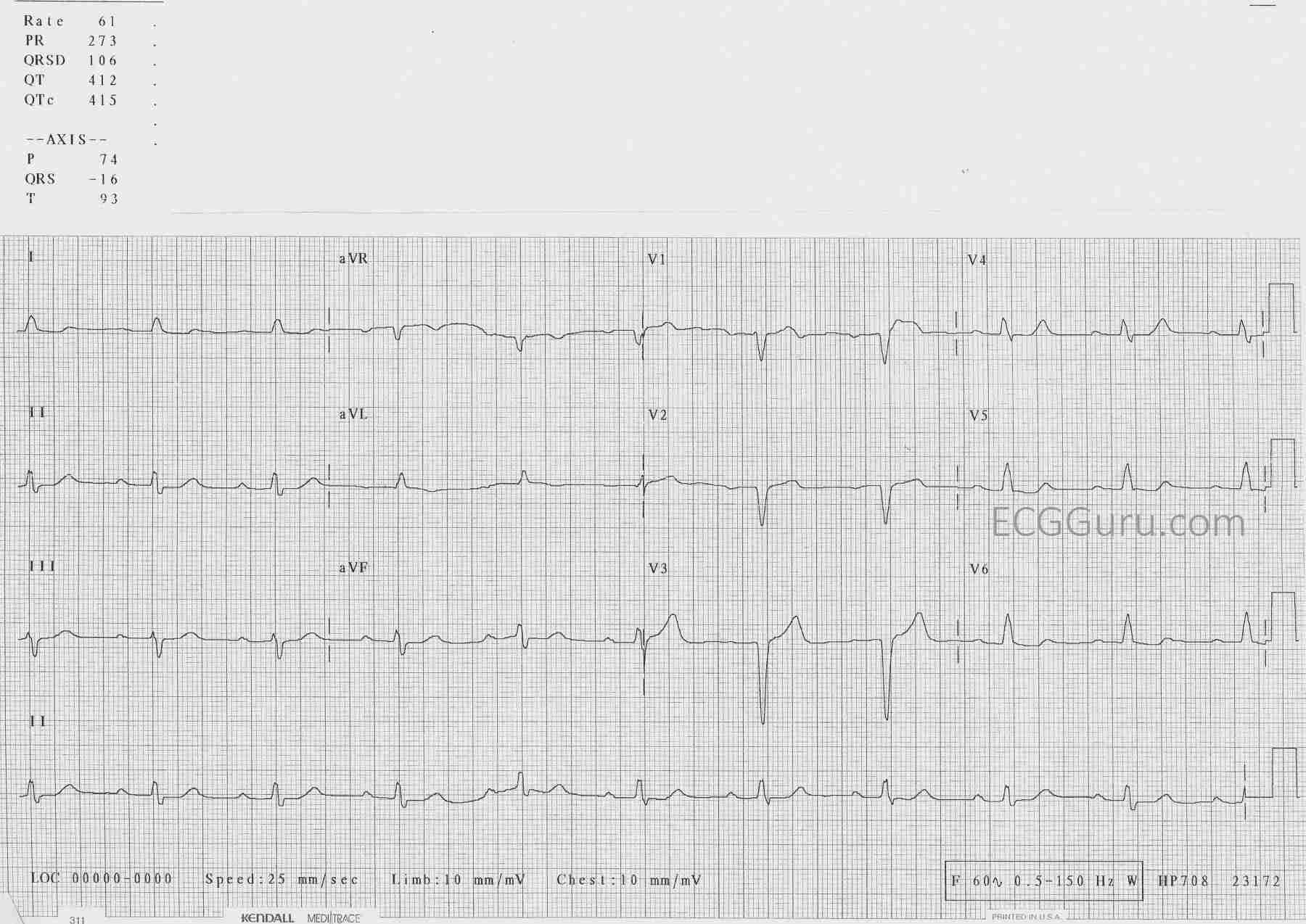
If you are an instructor, or a fairly new student, you don’t always need to see “challenging” ECGs. But, you may not want to see “standard” ECGs from an arrhythmia generator, either.Every ECG contains subtle and not, so subtle characteristics of the person it belongs to.Take a minute to look at this ECG before reading the discussion, and ask yourself what you might surmise about the patient.
The Patient: We don’t know much about the actual patient this ECG came from.What we do know is that he is an elderly man with a history of heart disease who was hospitalized sometime in the past with an acute M.I.He is now on beta blocker medication and is on a diet, as he is approaching the “morbidly obese” classification.He is now in the ER with shortness of breath and mild chest pain.What does his ECG tell us?
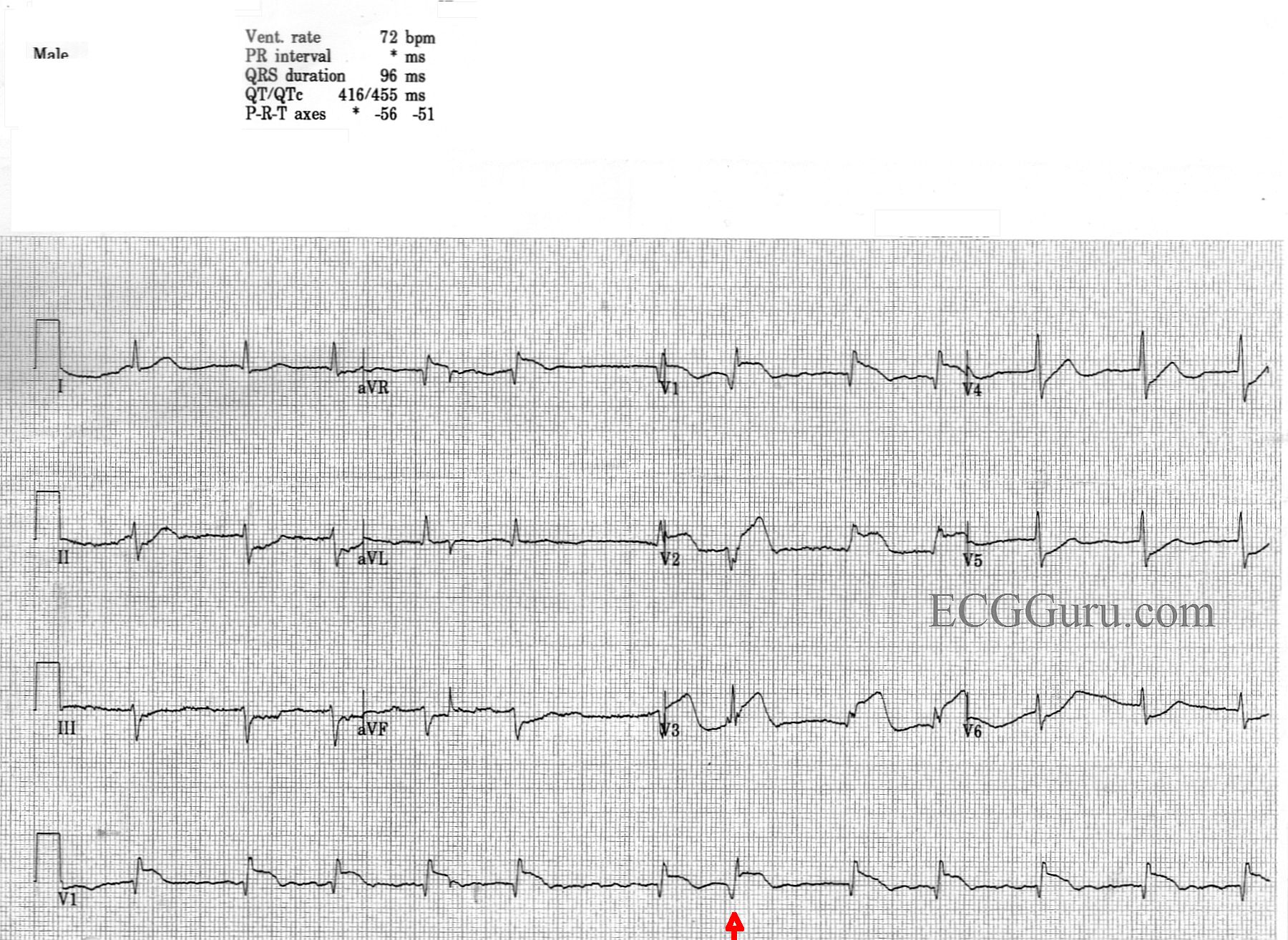
This is an interesting teaching ECG on many levels. It is obtained from a man with chest pain. No other history or follow up is available.
Acute M.I. Most striking is probably the clearly-seen anterior-septal wall M.I.There is ST segment elevation in Leads V1, V2, and V3, with ST depression in the low-lateral leads, V5 and V6.There is also ST depression in the inferior Leads II, III, and aVF.The ST elevations have a coved-upward (frown) shape in V1 and a straight shape in V2 and V3.Both of these ST shapes are abnormal and reflect injury.The depressions are presumed to be due to reciprocal changes, since there is no other ST-depression producing condition apparent.There are abnormal Q waves in V1, which could herald the onset of pathological Q waves, a sign of necrosis, in the anterior-septal wall.
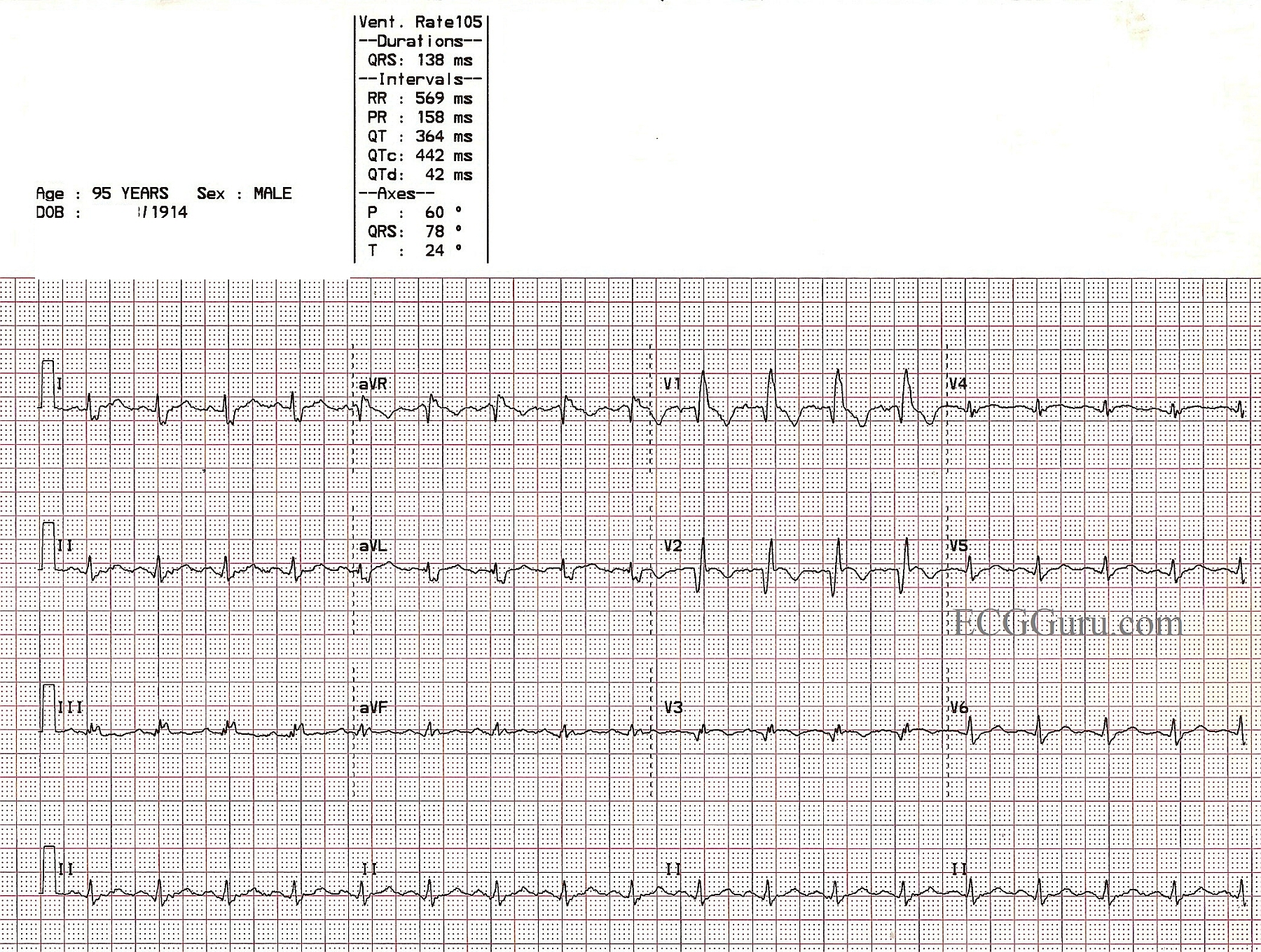
This is an ECG from a 95 year old man who was recovering from an anterior-septal wall M.I. Other clinical data for this patient has been lost, except that he suffered a new right bundle branch block during this M.I. The ECG shows pathological Q waves in V1, V2, and V3, consistent with permanent damage (necrosis) in the anterior septal wall. The ST segments in those leads are coved upward. Even though the J points are not elevated, this ST segment shape suggests recent injury. The classic RBBB pattern is present: wide QRS, rSR' pattern in V1, and wide little s waves in I and V6. It is not known why the overall voltage is low in this patient.