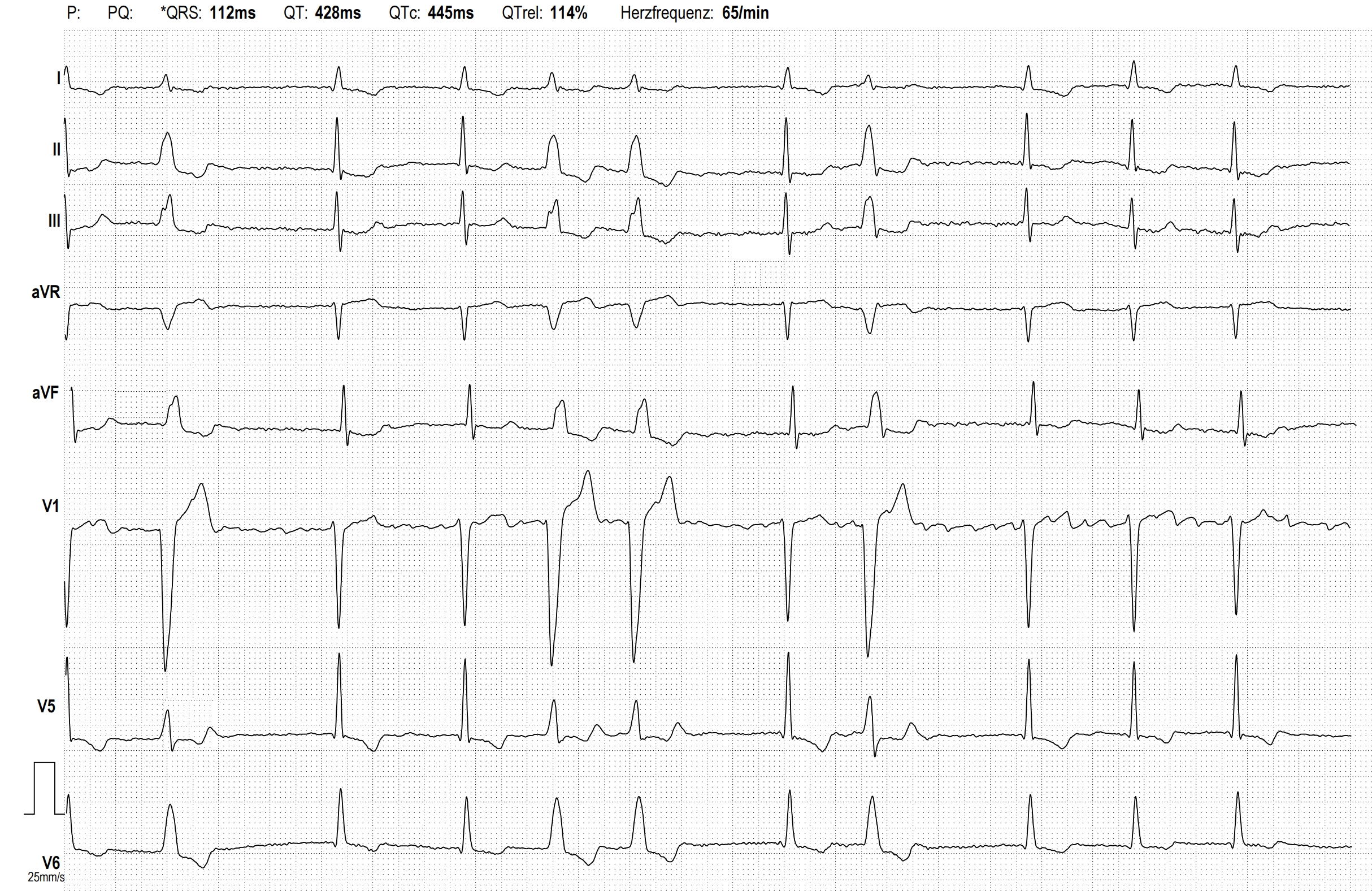
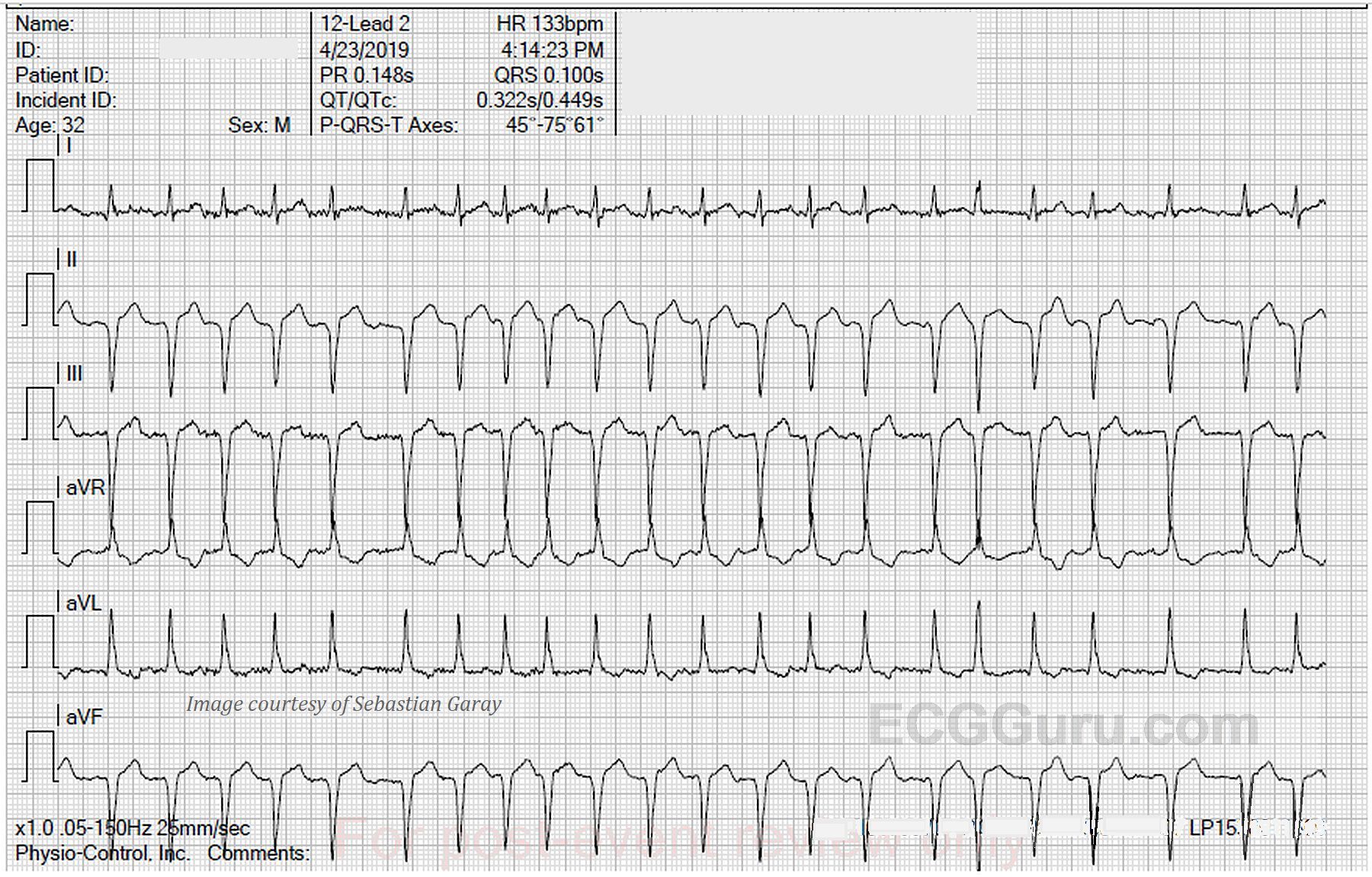
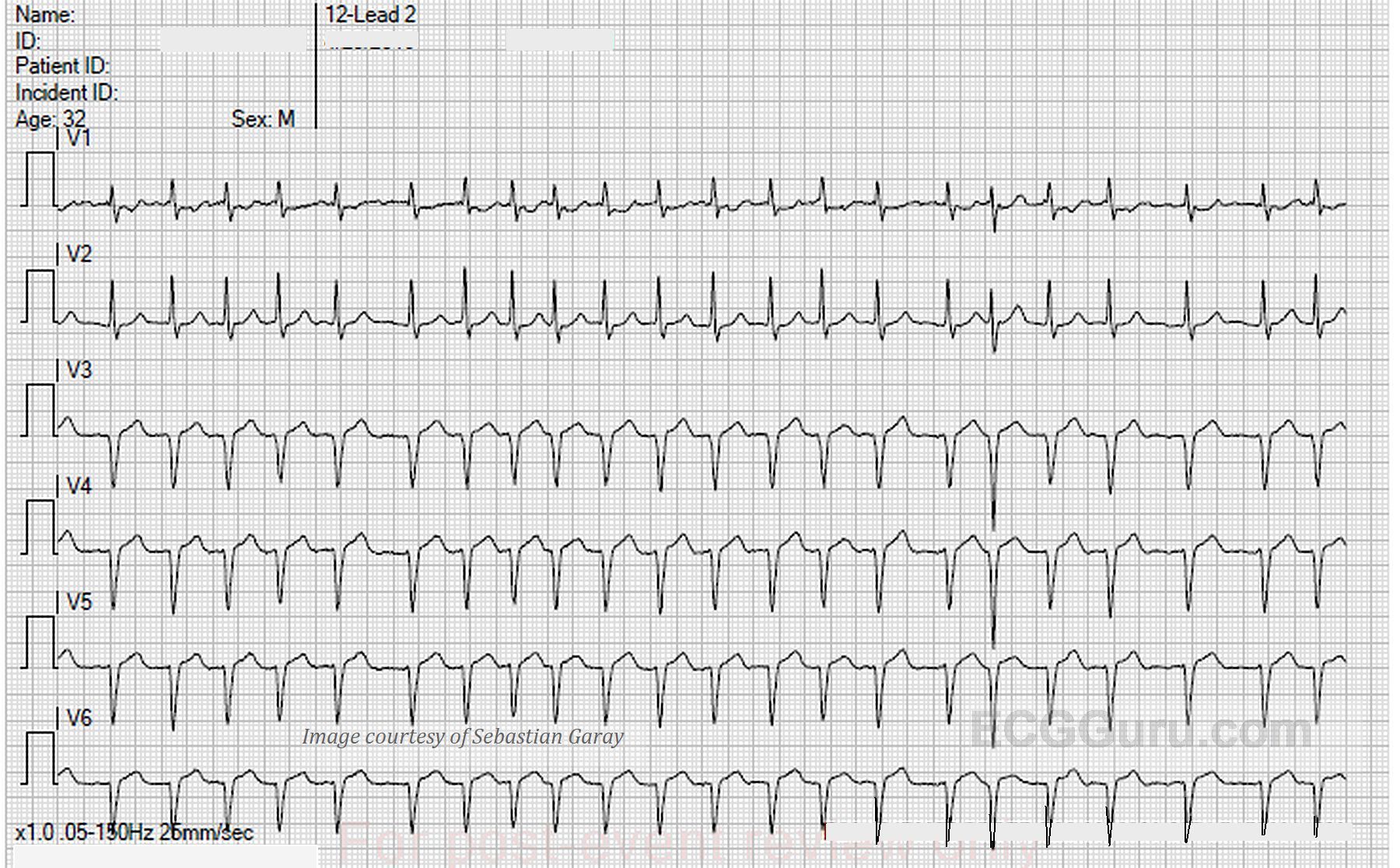
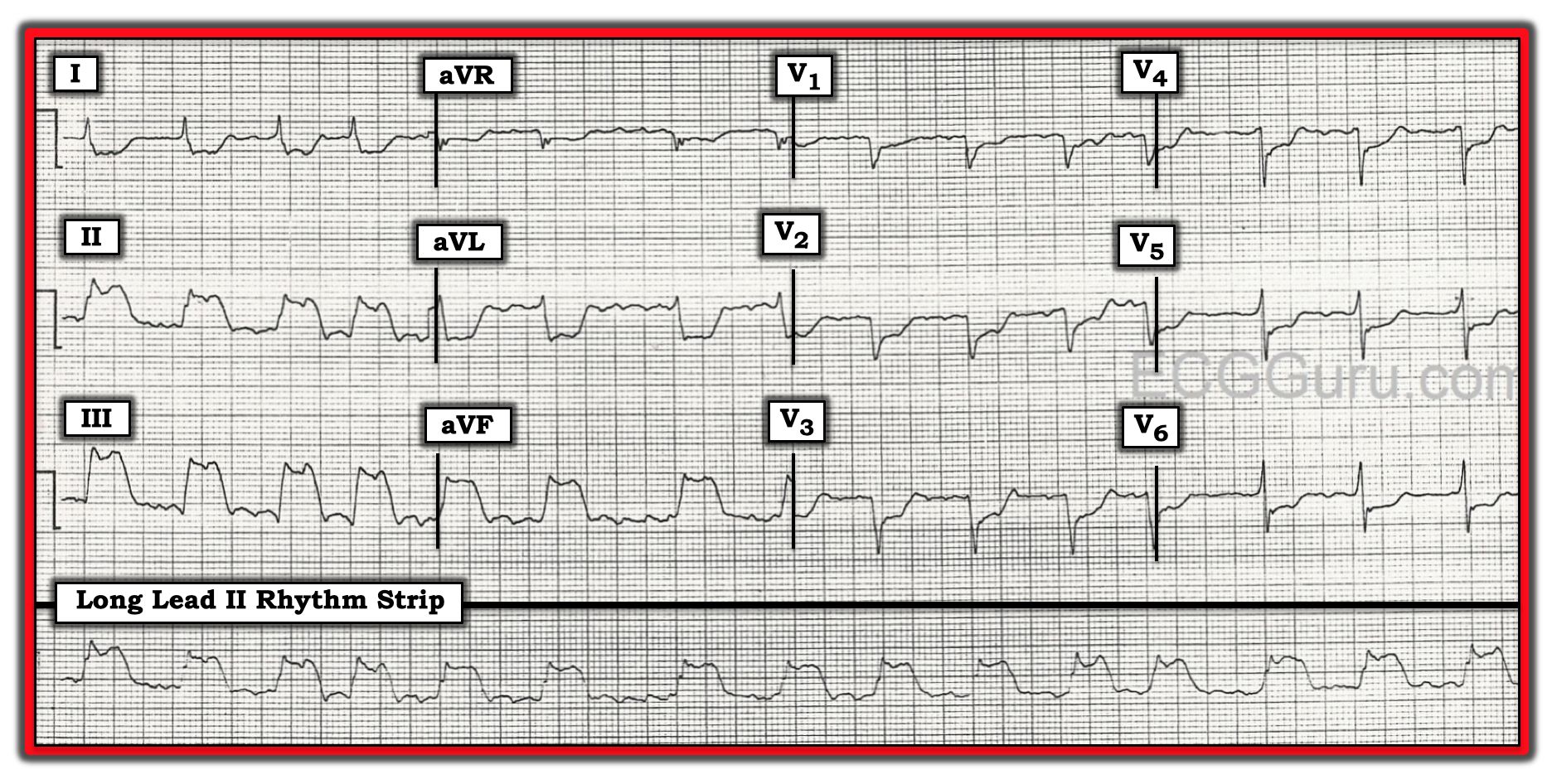
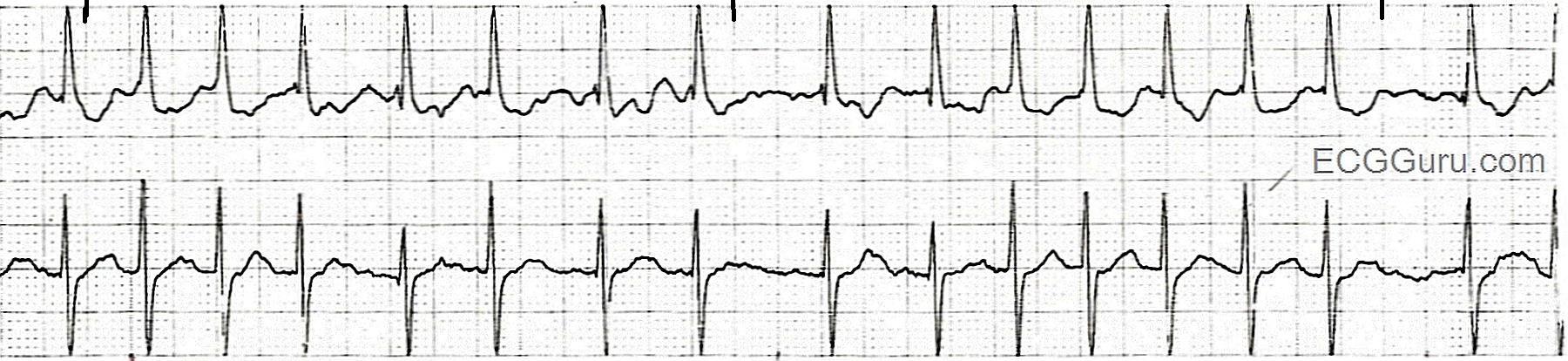
This strip shows the onset of atrial fibrillation. A fib can be "paroxysmal," meaning that it has a sudden onset, but then stops spontaneously, usually within 24 hours to a week. A fib can also be classified as "persistent", meaninging that the a fib lasts more than a week. It can stop spontaneously, or be halted with medical treatment. "Permanent" a fib is a fib that is resistent to treatment.
The first three beats in this strip represent sinus rhythm at 75 beats per minute. At the onset of atrial fibrillation with beat number four, the rhythm becomes irregularly irregular, and the rate is around 140-150 bpm. We can expect new-onset a fib to have a fast ventricular rate, as the atria are sending hundreds of impulses to the AV node every minute. The AV node will conduct as many of those impulses as it can to the ventricles. Most AV nodes can easily transmit 130-160 bpm. In a fib, the atria are quivering, not contracting. Because of this fibrillation of the atrial muscle, a fib has no P waves, and therefore, no "atrial kick". The contribution of the atria to cardiac output (25-30%) is lost. An extremely fast rate can also lower output and overwork the heart, so one treatment goal for a fib is to lower the rate. This can be done independently of attempts to convert the rhythm.
During a fib, blood clots can form in parts of the atria, especially the left atrial appendage. If sinus rhythm is restored after these thrombi form, they can embolize and travel to the brain, causing stroke. Before electively converting atrial fib to a sinus rhythm, the patient may need to be anticoagulated.