The Patient
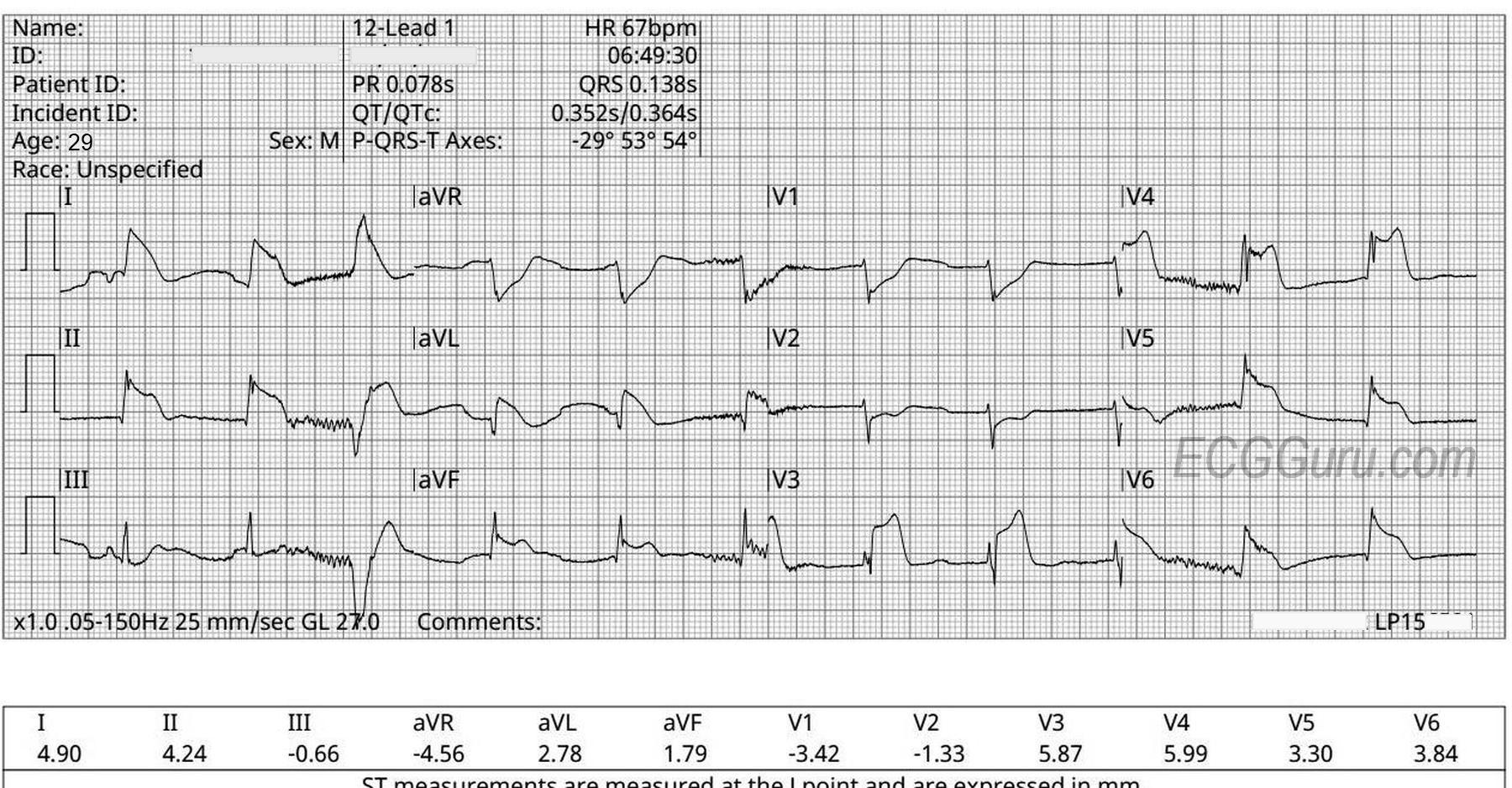
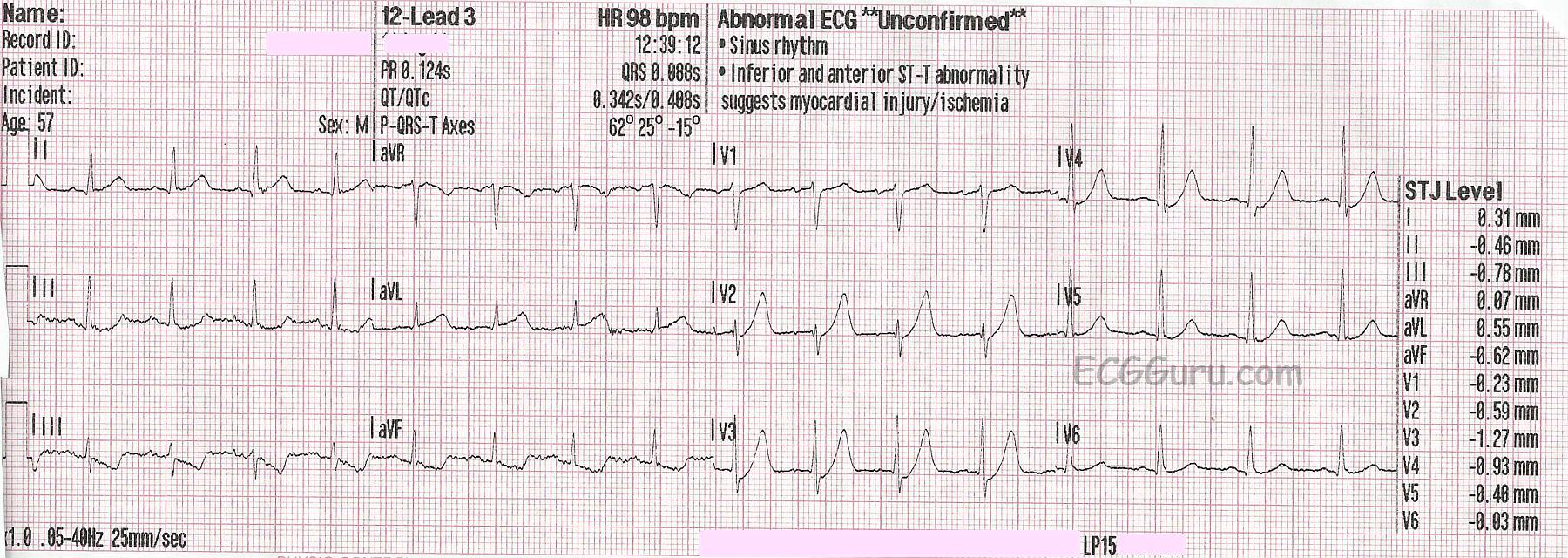
This ECG is from a 57-year-old man complaining of sub-sternal chest pain for 30 minutes. EMS found him pale, diaphoretic, and anxious. We don't have other clinical information or past medical history.
The ECG
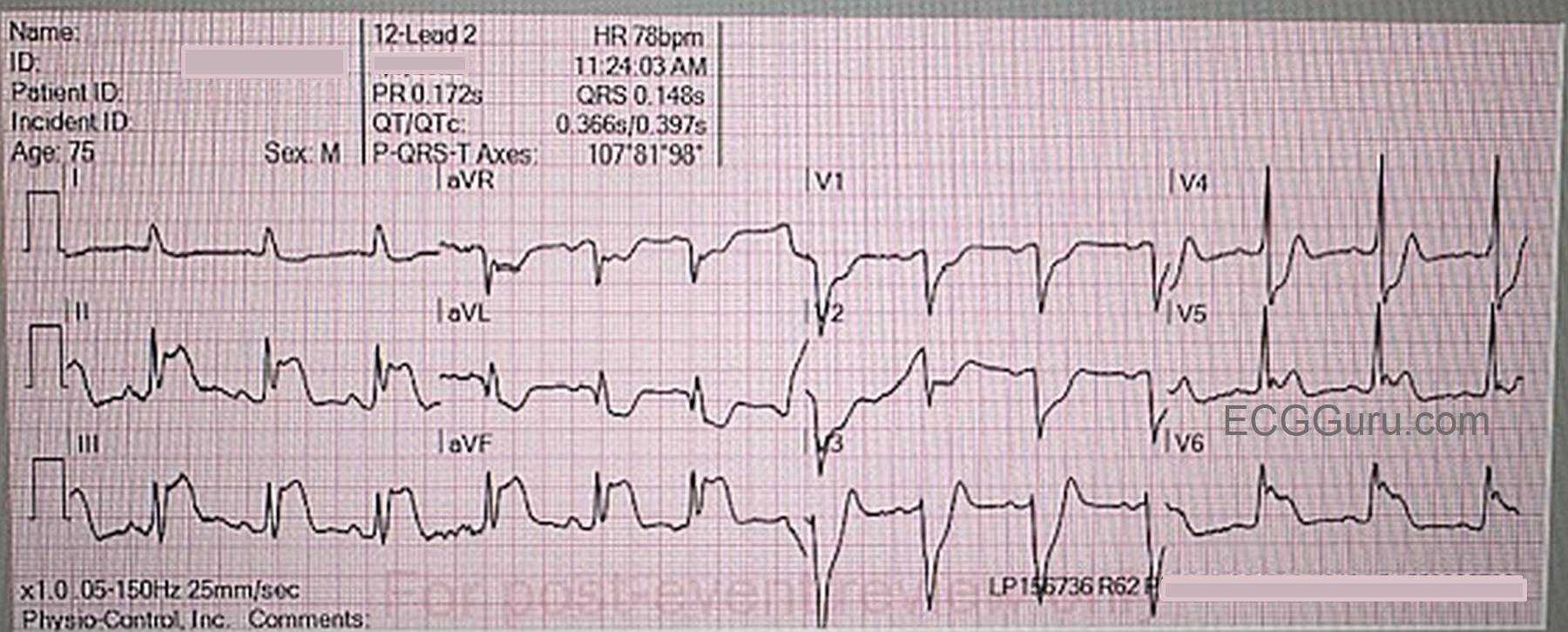
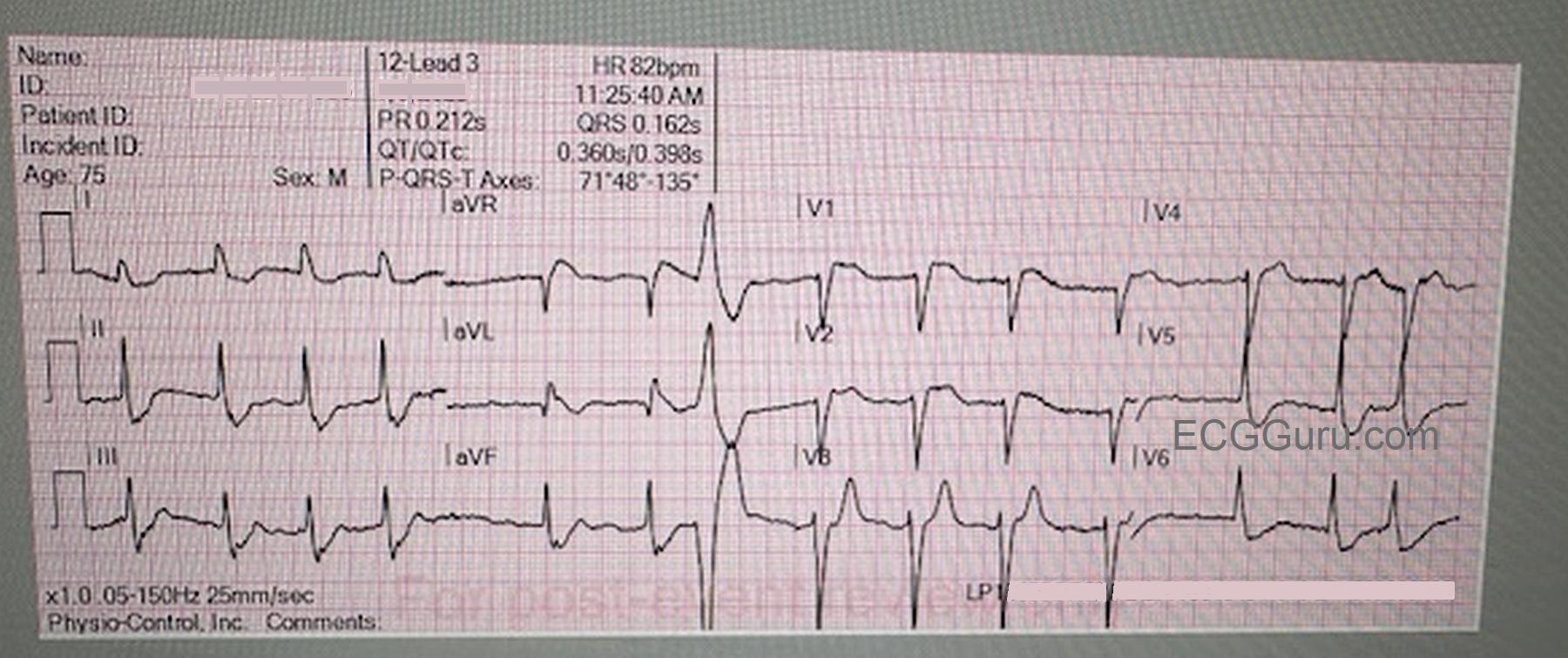
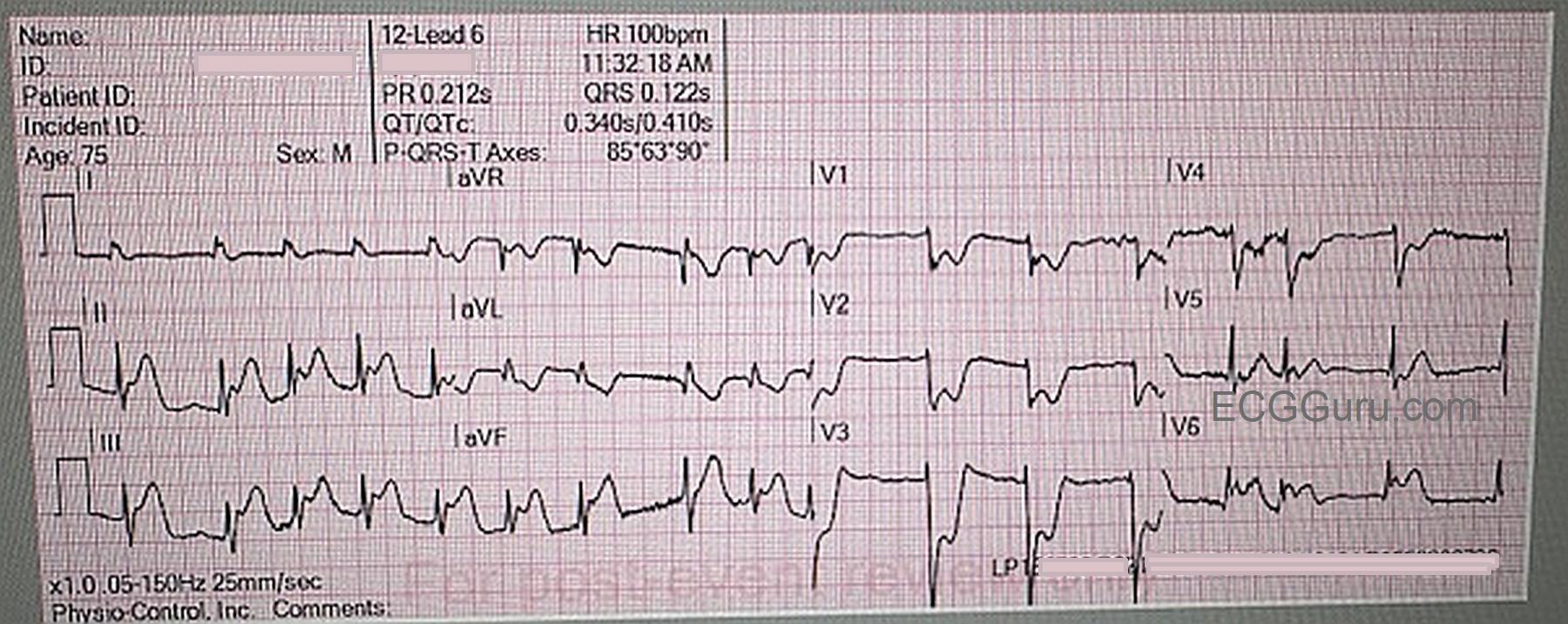
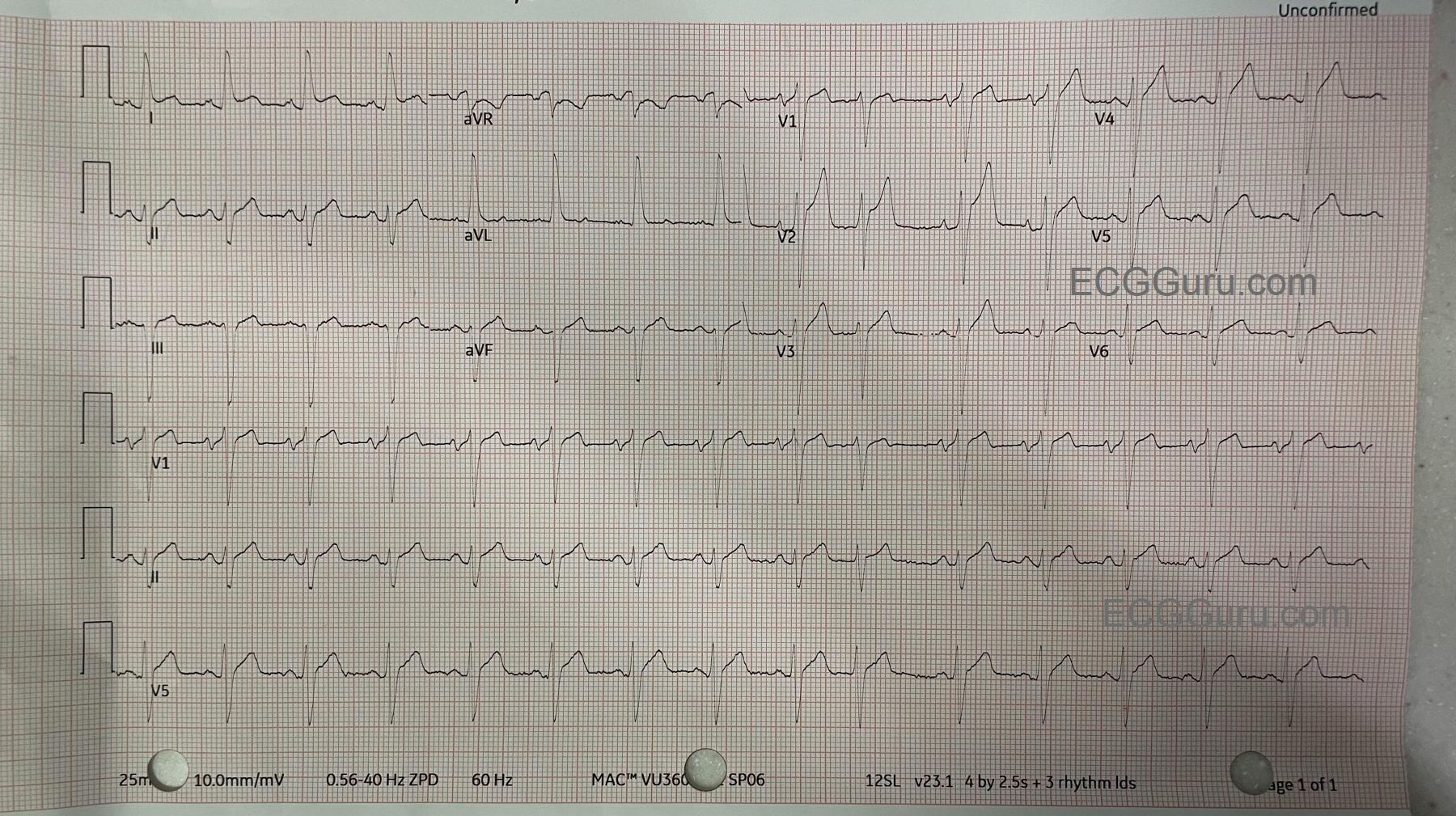
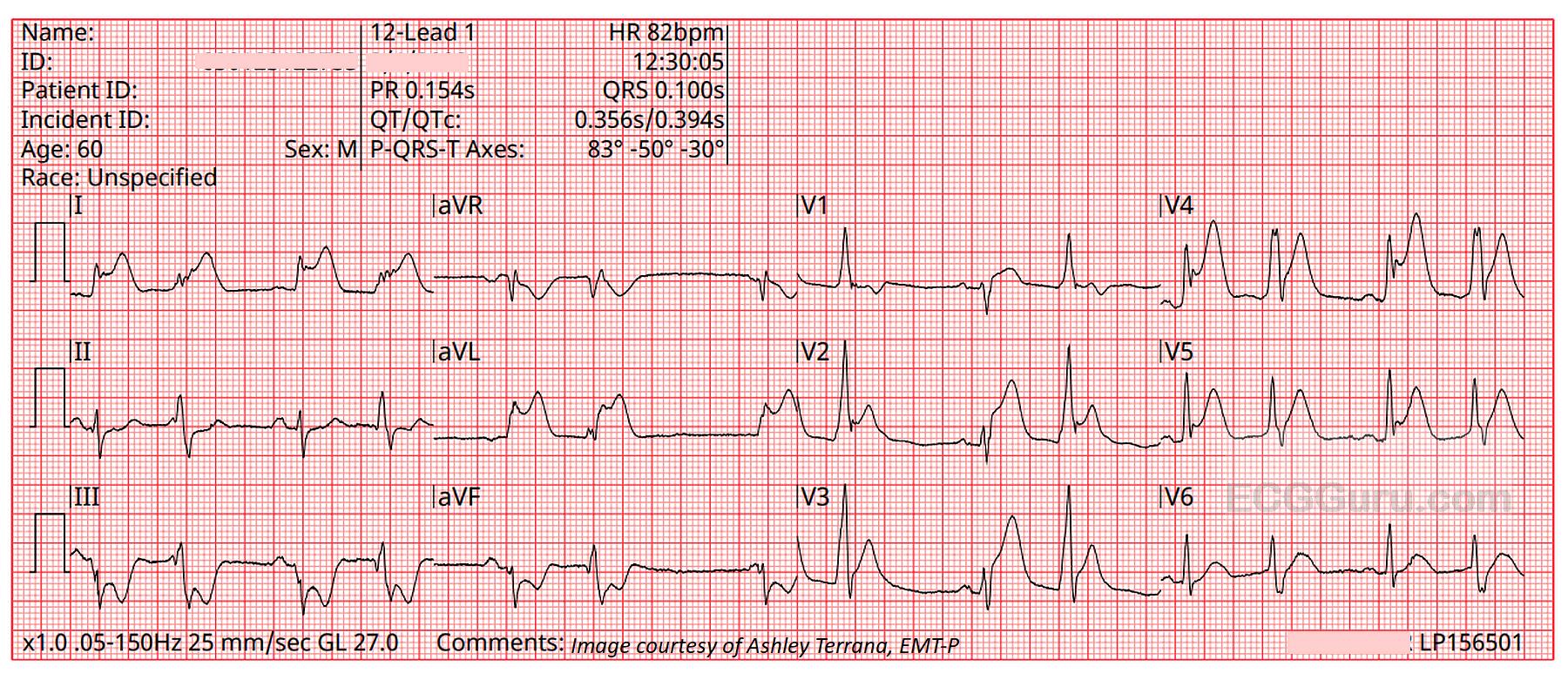
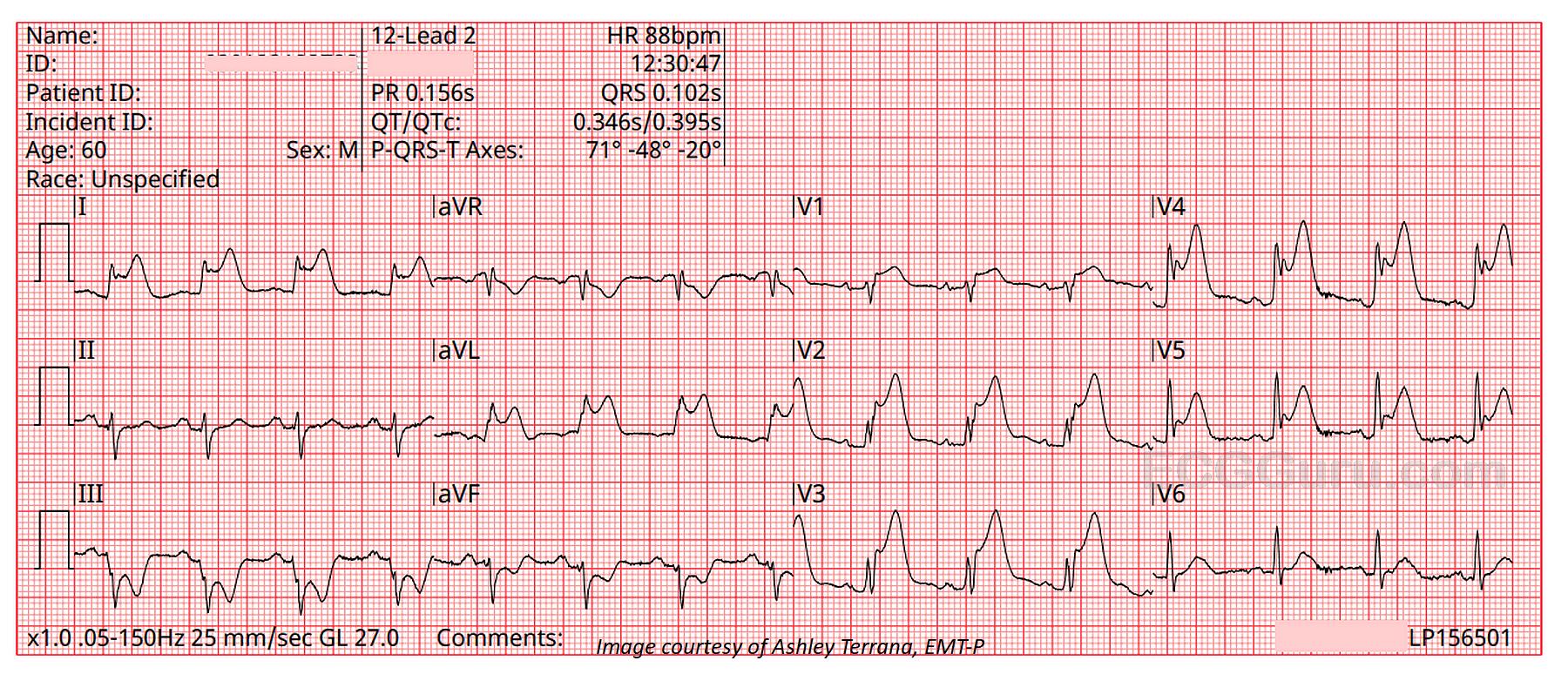
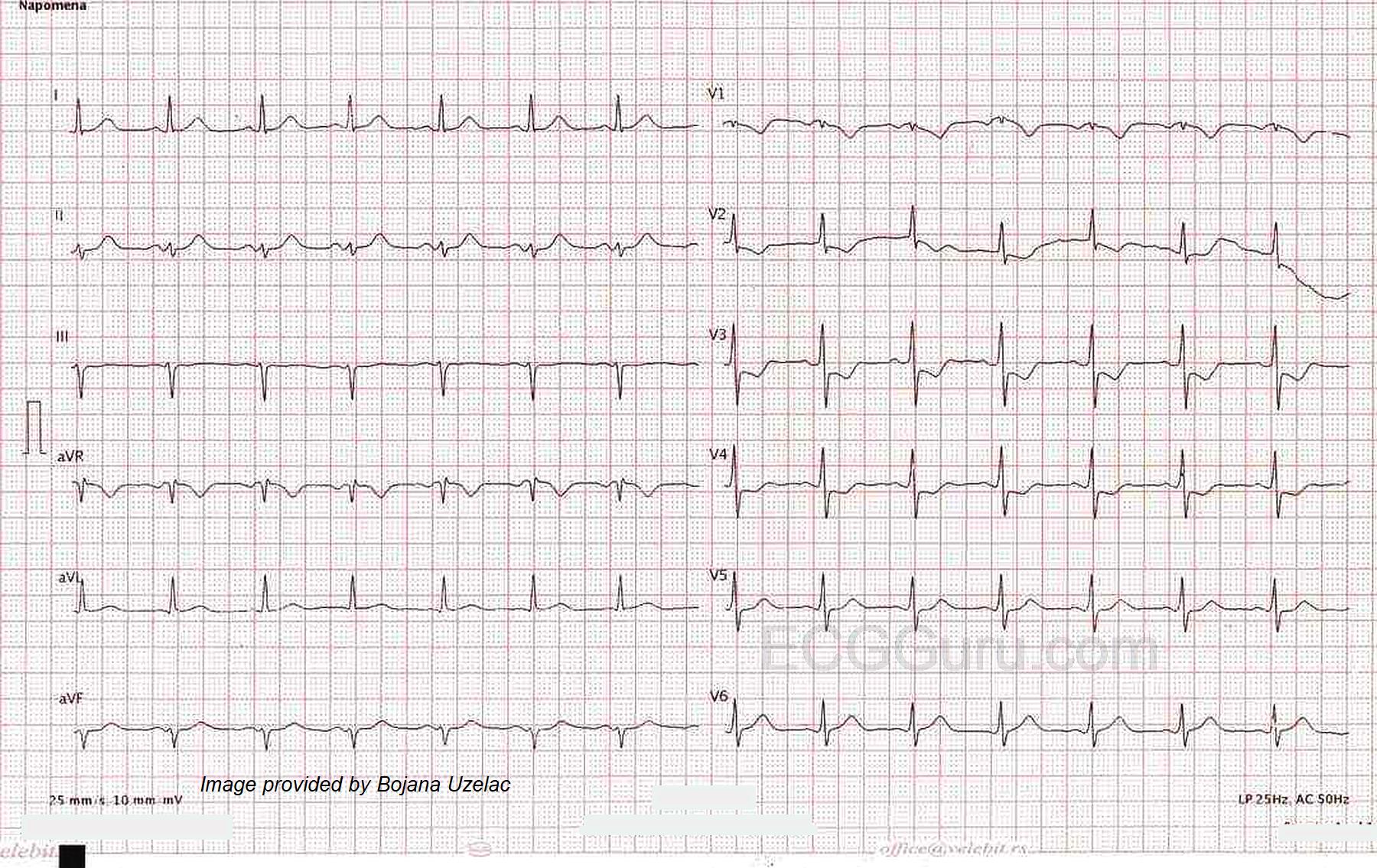
The rhythm is normal sinus rhythm at 98 bpm. The QRS is narrow, and the PR and QTc intervals are within normal limits. In precordial leads V2 through V4, ST segments begin at a J point that is below the baseline by one small block (the computer reads all precordial leads as having a small J point depression). From those depressed J points, there are upsloping ST segments leading into hyperacute T waves.
This is called de Winter T wave pattern, and it is a sign of critical proximal occlusion of the left anterior descending coronary artery. Dr. Robbert de Winter, et al, described this pattern in a letter to the editor of the New England Journal of Medicine in 2008. Since then, it has been estimated to occur in about 2%-3.4% of acute occlusive myocardial infarctions. It has been seen in occlusions of other major arteries, but by far most cases are seen in LAD occlusion. This should not be considered to be an "impending M.I.", but rather a STEMI equivalent, warranting emergent treatment in a cath lab.
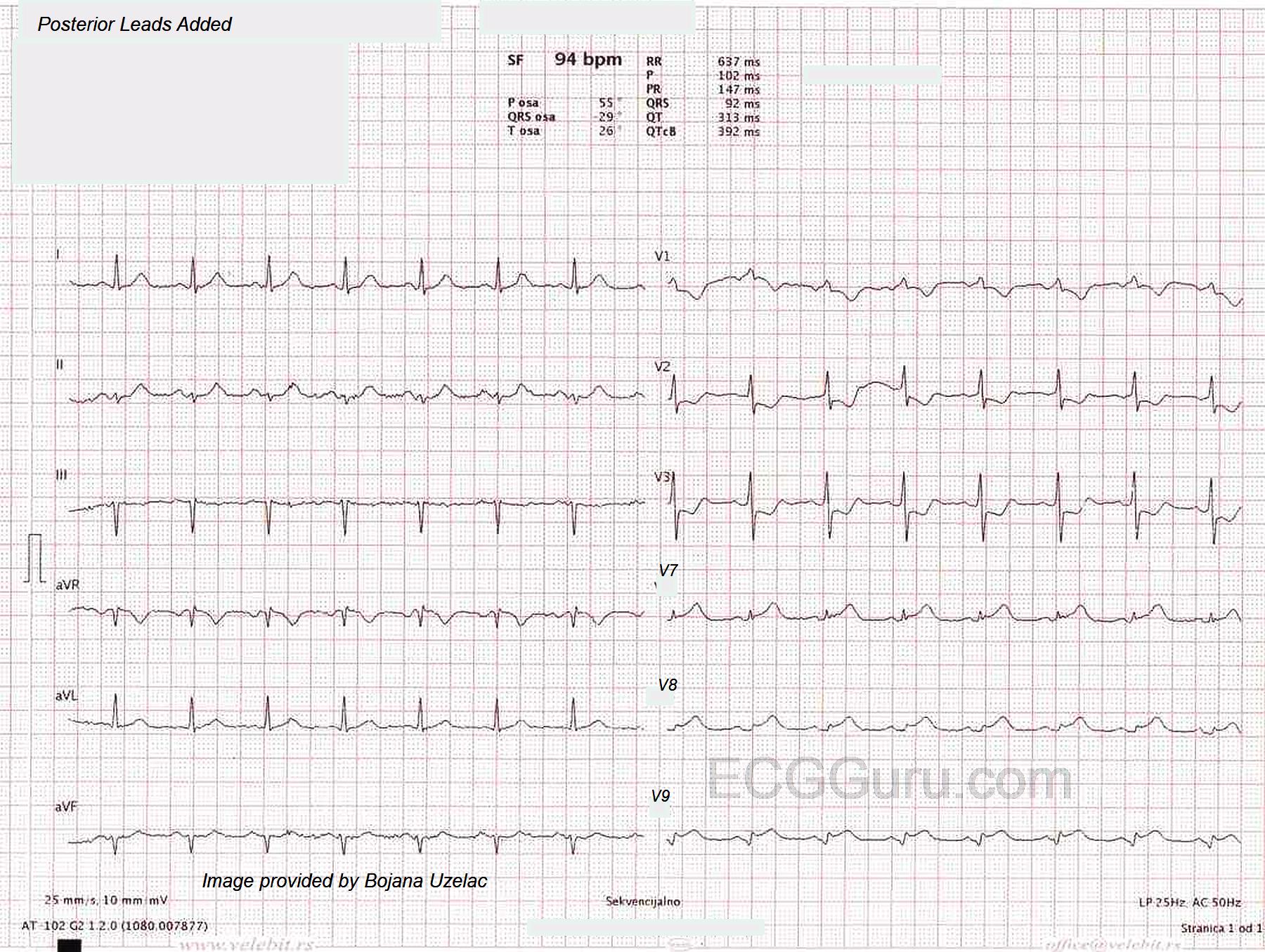
In this ECG, we see a curving upward of the ST segment in aVR, with very slight STE noted by the computer. ST elevation in aVR is a common finding with proximal LAD occlusion. There is also subtle ST elevation in I and aVL with reciprocal ST depression in II, III, and aVF without hyperacute T waves, common when the occlusion is so proximal it affects the obtuse marginal branch of the circumflex or first diagonal branch of the LAD.
The J point changes of the de Winter pattern are seen with hyperacute T waves. T waves are considered hyperacute if they are larger than normal for the lead they are seen in. When we say, "large", it refers more to the width of the base of the T waves, and the space contained within the T wave, although they can be quite tall sometimes. A tall, but narrow and pointed T wave would be more indicative of hyperkalemia than of de Winter pattern.
Follow up
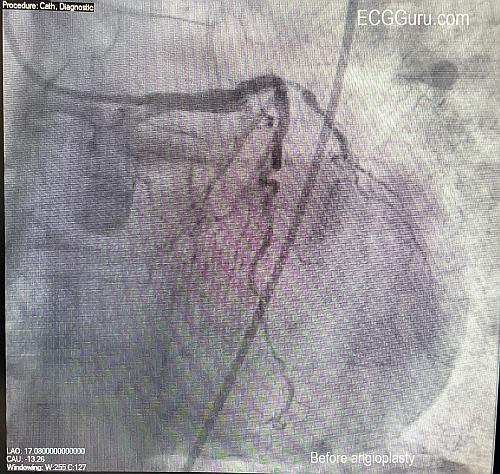
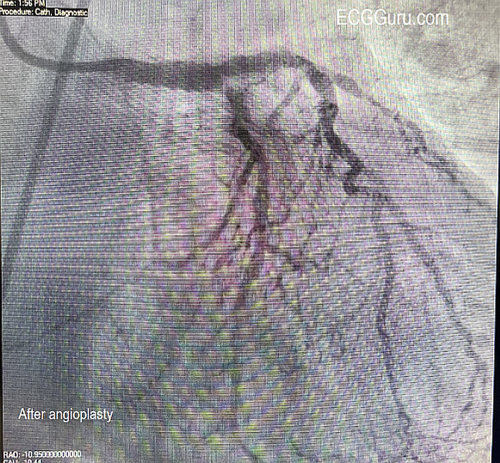
Unfortunately, we don't have follow up information on this patient, other than he arrived at the Emergency Department alive and was scheduled for the cath lab.