The Patient: These tracings are taken from a 75-year-old man who became weak while playing golf on a very hot day. He was pale and diaphoretic. He was hypotensive, but we do not know his BP reading. He denies chest pain or discomfort. The patient reported a history of lung cancer and hypertension. We have no other history, and unfortunately, no follow-up information.
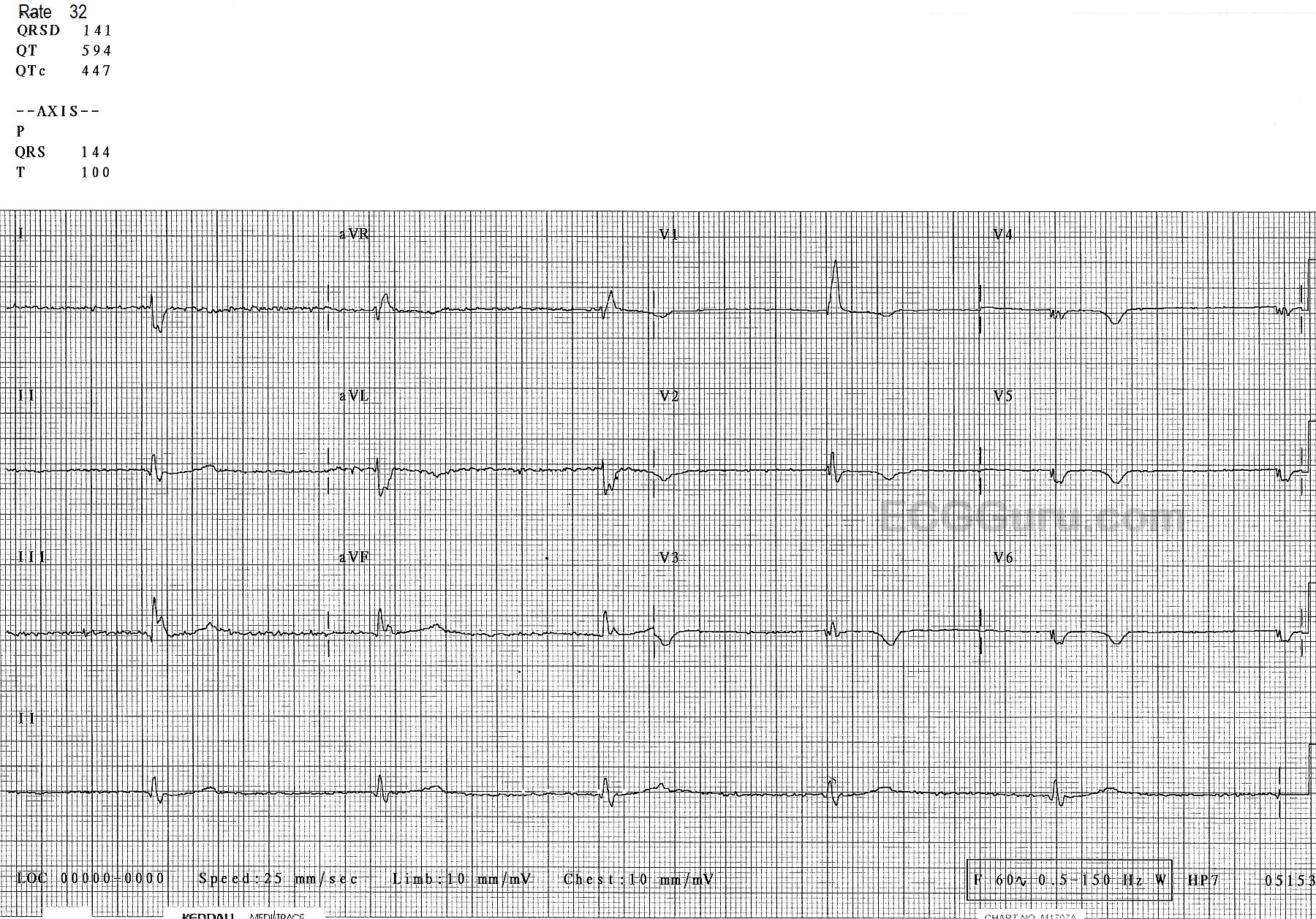
ECG Number 1: The first ECG shows the standard 12 leads. The rhythm is sinus with frequent appearances of PAC couplets. The sinus rate varies slightly from about 76 bpm to 68 bpm, tending to slow a bit after the premature atrial contractions. There is a right bundle branch block, and the QRS duration is about .12 seconds (120 ms). The PR interval is slightly log at 223 ms. We do not know what medications the patient is on, and we do not have an older ECG for comparison.
There are some interesting, if subtle, changes worth mentioning. The QRS complexes in most leads are fragmented. That is, they have notching in the terminal S or R waves that is not due to the bundle branch block. This can be a sign of scarring, and can also be considered an equivalent to a pathological Q wave. Speaking of pathological Q waves, they are seen in the inferior leads, II, III, and aVF. There are also prominent, though not large Q waves in V4 through V6, leads which normally do not have them. All this points to scarring and possibly long-term coronary artery disease, with possible old M.I. In addition, the ST segments are not entirely normal. There is ST depression in the inferior and low lateral leads, a little ST elevation in aVL. Also, the SHAPES of the ST segments tend to be straight throughout the ECG, instead of the usual curved (concave up) appearance.