The Patient: A 78-year-old woman called emergency responders because she had palpitations. She was alert and oriented. Her BP was reported as being “stable”. We do not have information about her past medical history. We will update this post if we receive information about her outcome.
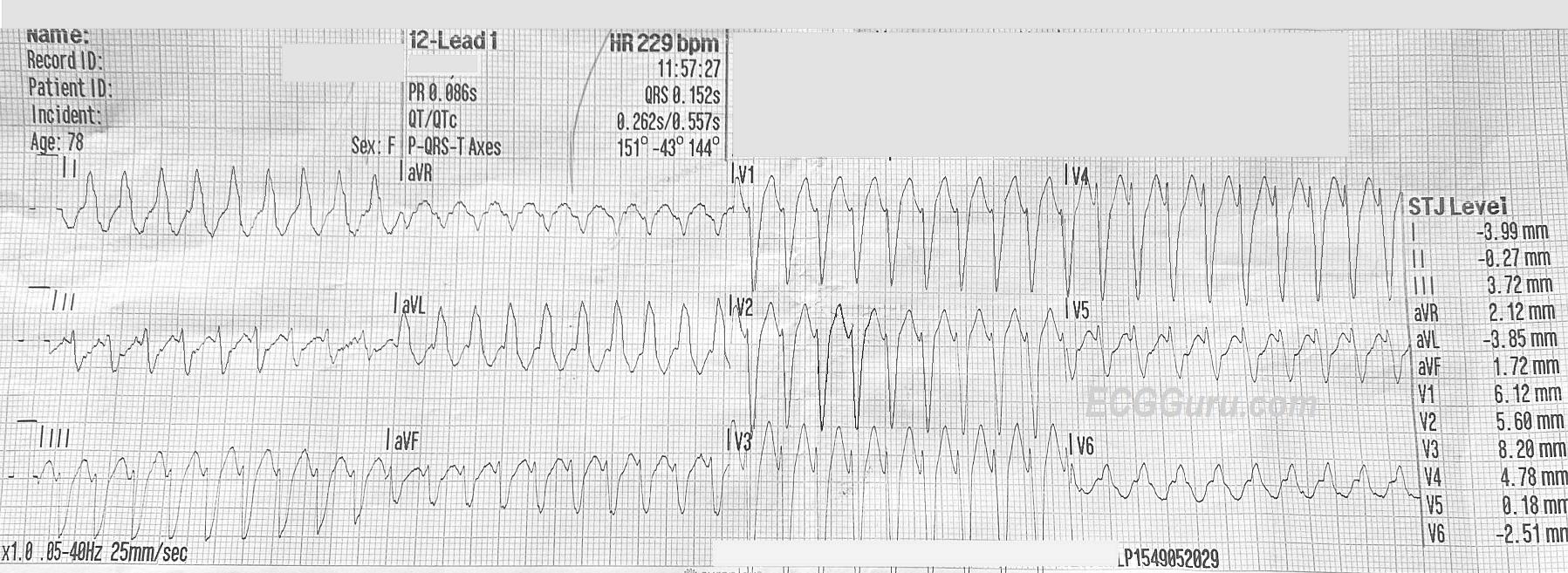
ECG Number 1, 11:57 a.m.: There is a wide-complex tachycardia at a rate of about 230 bpm. The QRS is .15 seconds (150 ms). The QRS frontal plane axis is leftward. P waves are not readily seen, but the computer gives a P axis and PRI. The PRI given is taken from Lead II, which, along with V5, does have P waves. In the other leads, the P waves are buried in preceding T waves. This photo shows an ECG that is not lying flat, so it is difficult to line up the complexes. Normally, it helps to look at the leads above or below to determine where waves begin and end, as all three channels are run simultaneously. The QRS complexes have a “typical” left bundle branch block morphology, with an rS complex in V1 and a monophasic R wave in Leads I and V6. The T waves are “discordant”, they are in the opposite direction from the QRS complexes, which is typical of LBBB.
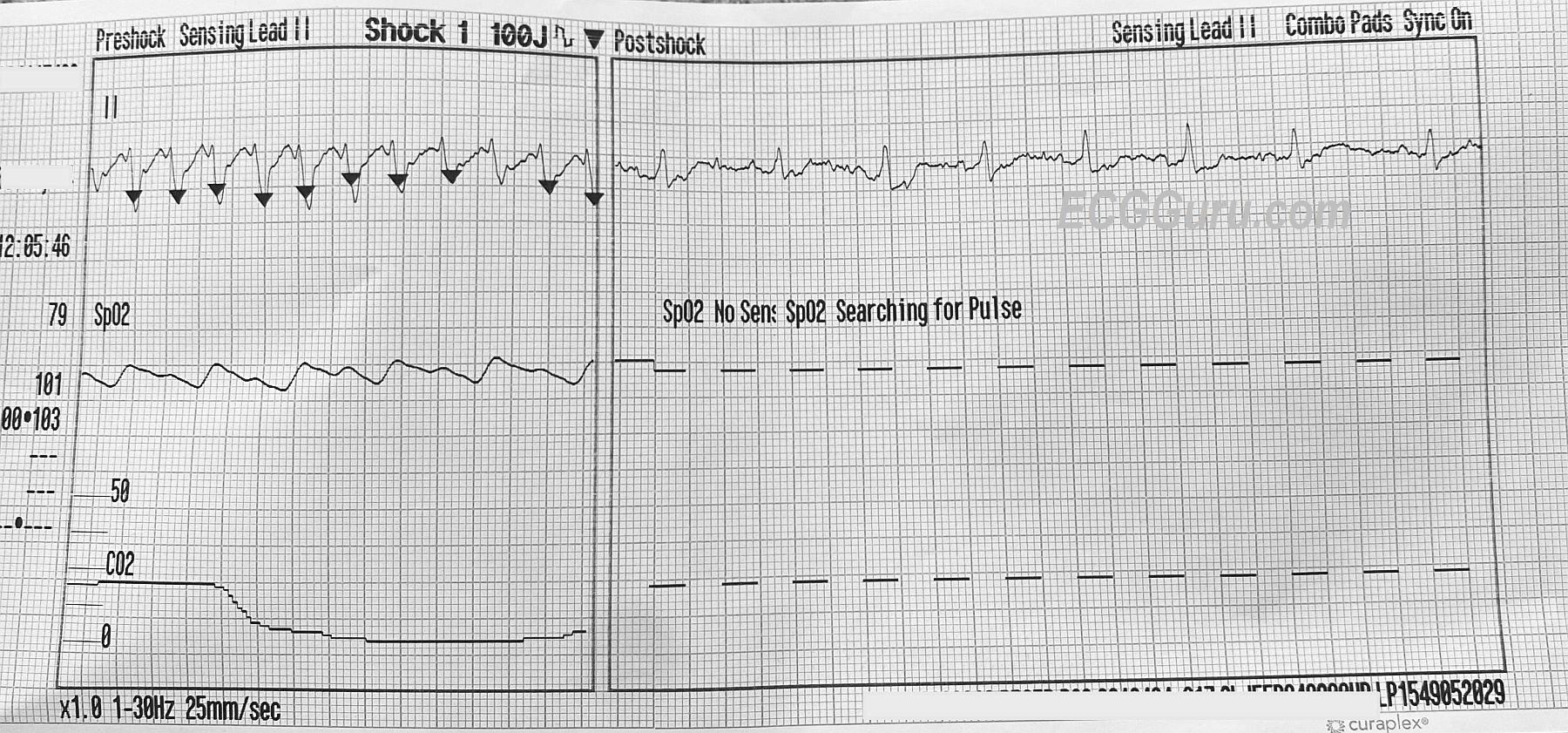
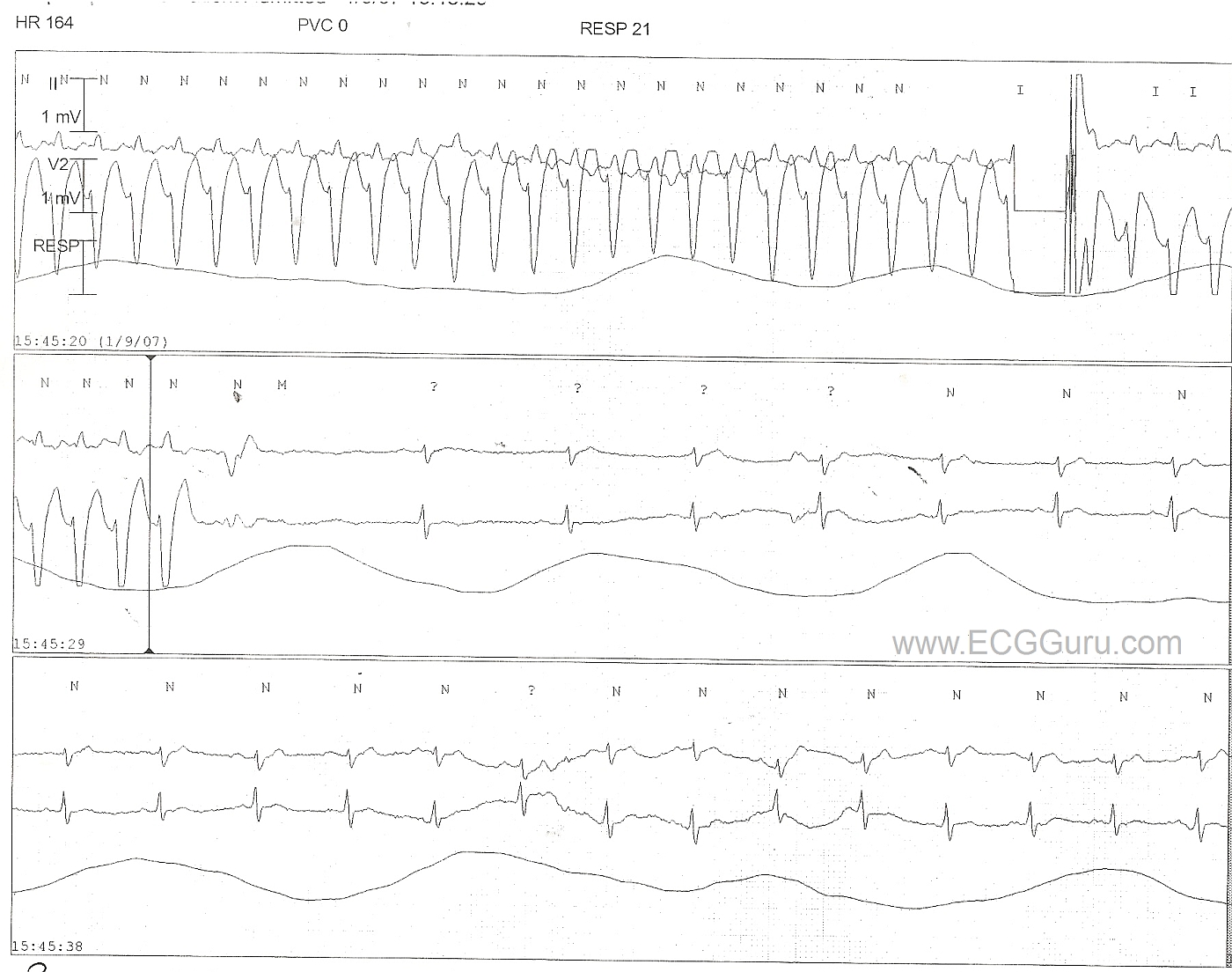
ECG Number 2, 12:05 p.m.: This is a rhythm strip recording a synchronized shock at 100 joules, resulting in conversion of the WCT to a narrow complex, irregular rhythm. It appears that there is a P wave before every narrow QRS, but artifact prevents proper evaluation.