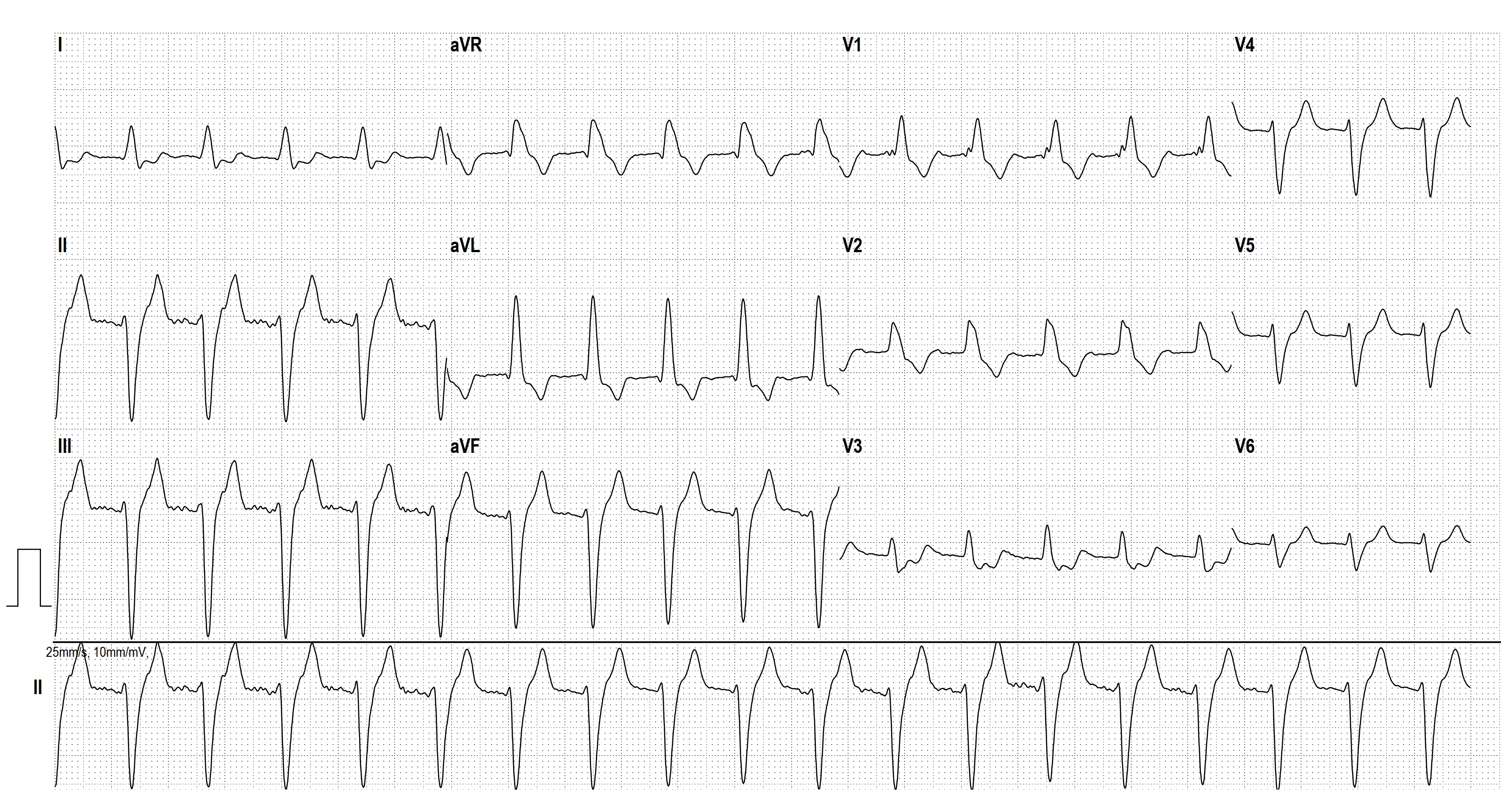
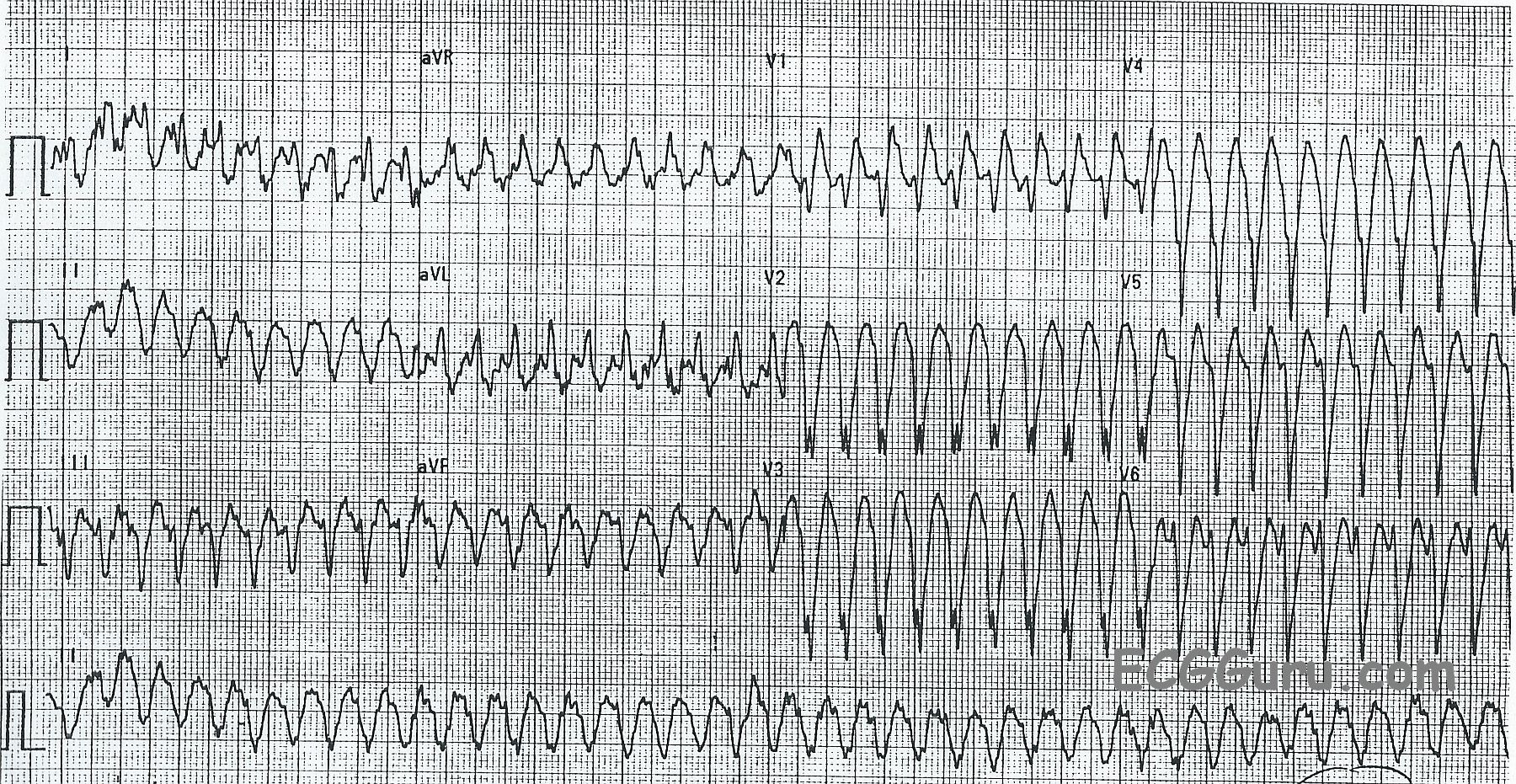
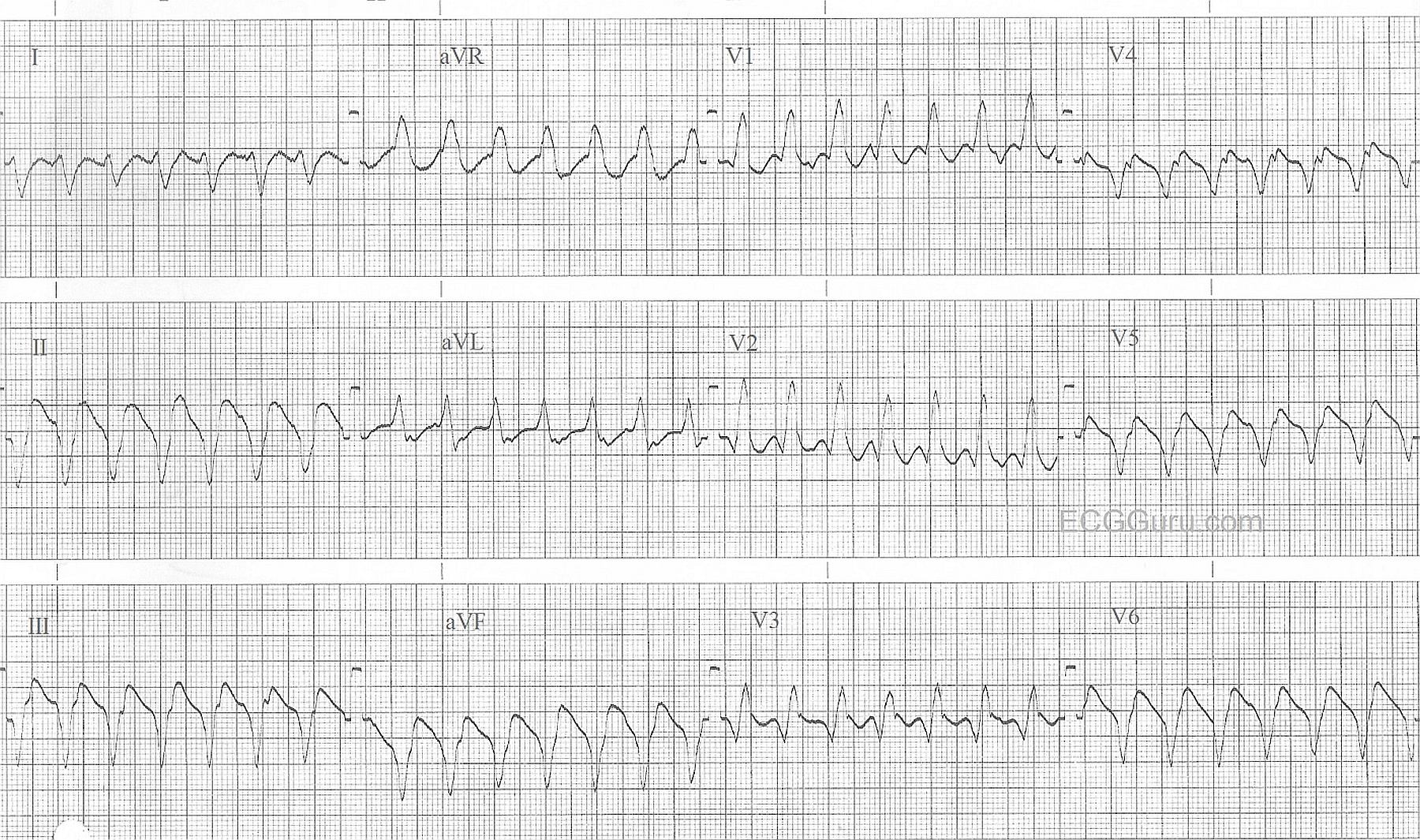
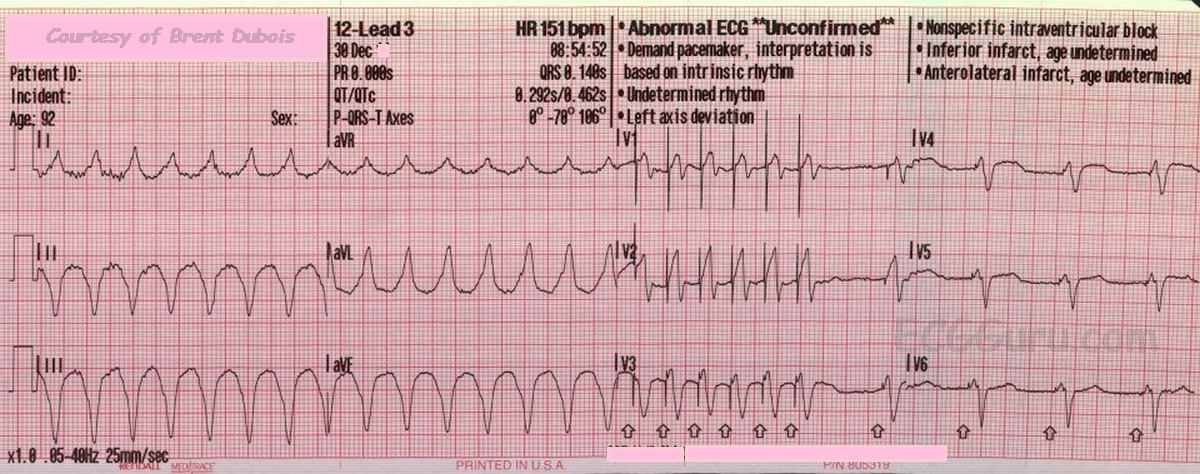
This ECG is from a man who was experiencing palpitations and light-headedness with near-syncope. On first look, you will see a wide-complex tachycardia (WTC) with a rate around 240 per minute. It is difficult to assess for the presence of P waves because of the rate and the baseline artifact.
The differential diagnosis of WCT includes ventricular tachycardia and supraventricular tachycardia with aberrant conduction, or interventricular conduction delay (IVCD). We should ALWAYS consider VENTRICULAR TACHYCARDIA first. If the patient is an older adult with structural heart disease, WCT almost always proves to be VT.
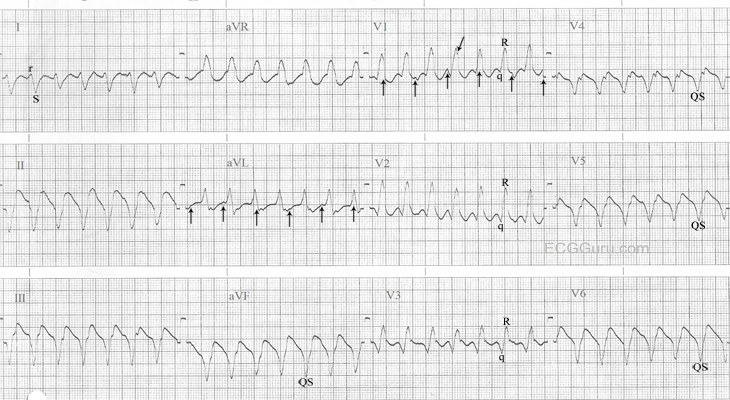
ABERRANT SVT? In the setting of SVT with wide QRS, the most common aberrancy is right or left bundle branch block. This ECG could be said to have a “RBBB” type pattern in V1, rSR’ and in Lead I and V6 with a wide S wave. However, the other precordial leads do not have a RBBB pattern.
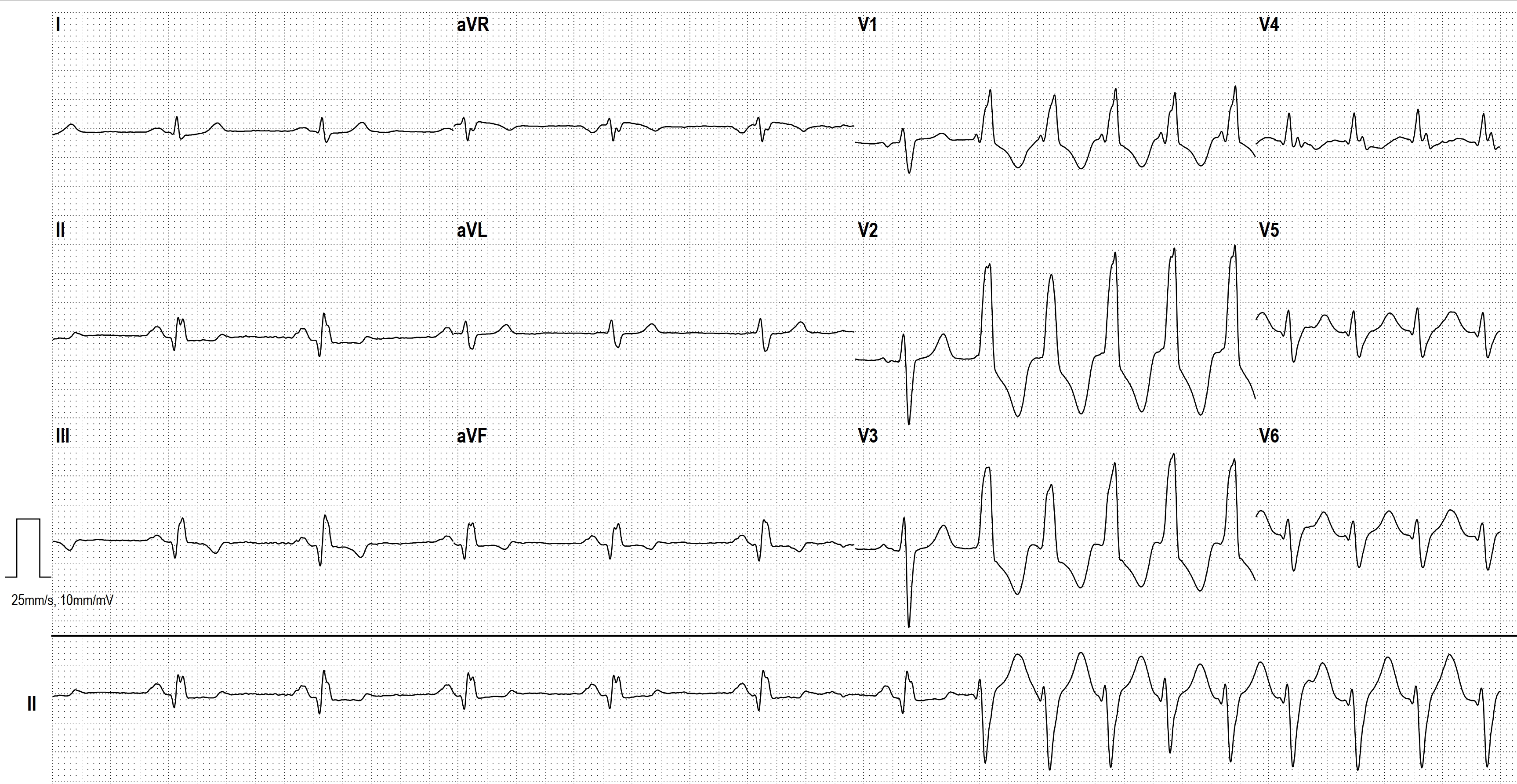
VENTRICULAR TACHYCARDIA? There are some features of this ECG that favor the diagnosis of VENTRICULAR TACHYCARDIA (VT). They include, but are not limited to:
* Regular, wide QRS complexes, about .14 seconds in this ECG, but varies because of difficulty in measuring the beginning and end of the QRS in each lead. The artifact obscures the exact points of beginning and ending. The QRS complexes, especially from V2 leftward, are very “ugly”, and don’t resemble patterns we would expect with bundle branch block.
* Horizontal plane axis extremely abnormal: Leads II, III, and aVF are negative and aVR and aVL are positive. The biphasic Lead I indicates a nearly vertical axis at around – 90 degrees.
* There is “almost” precordial concordance, but V1 is biphasic.
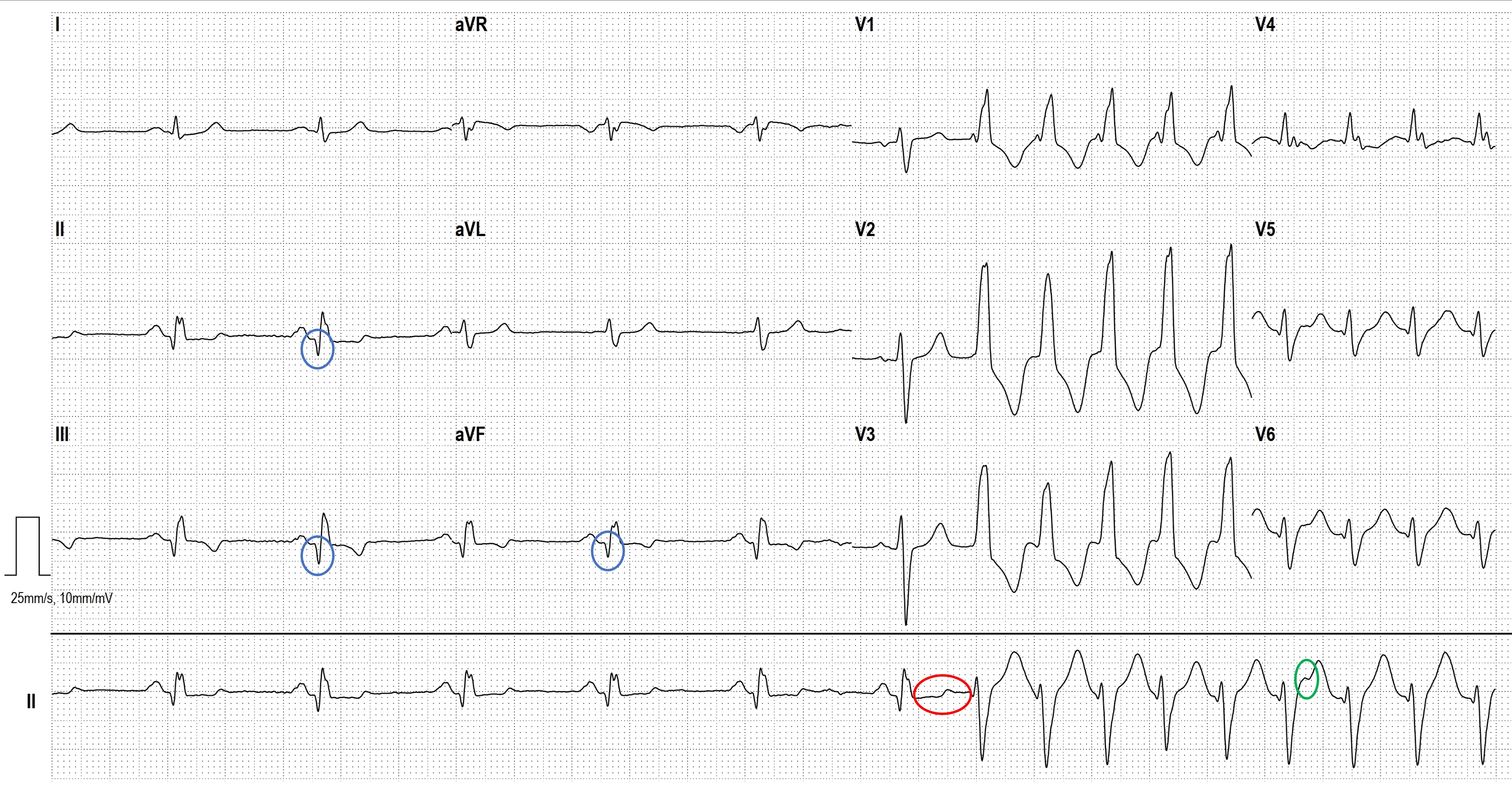
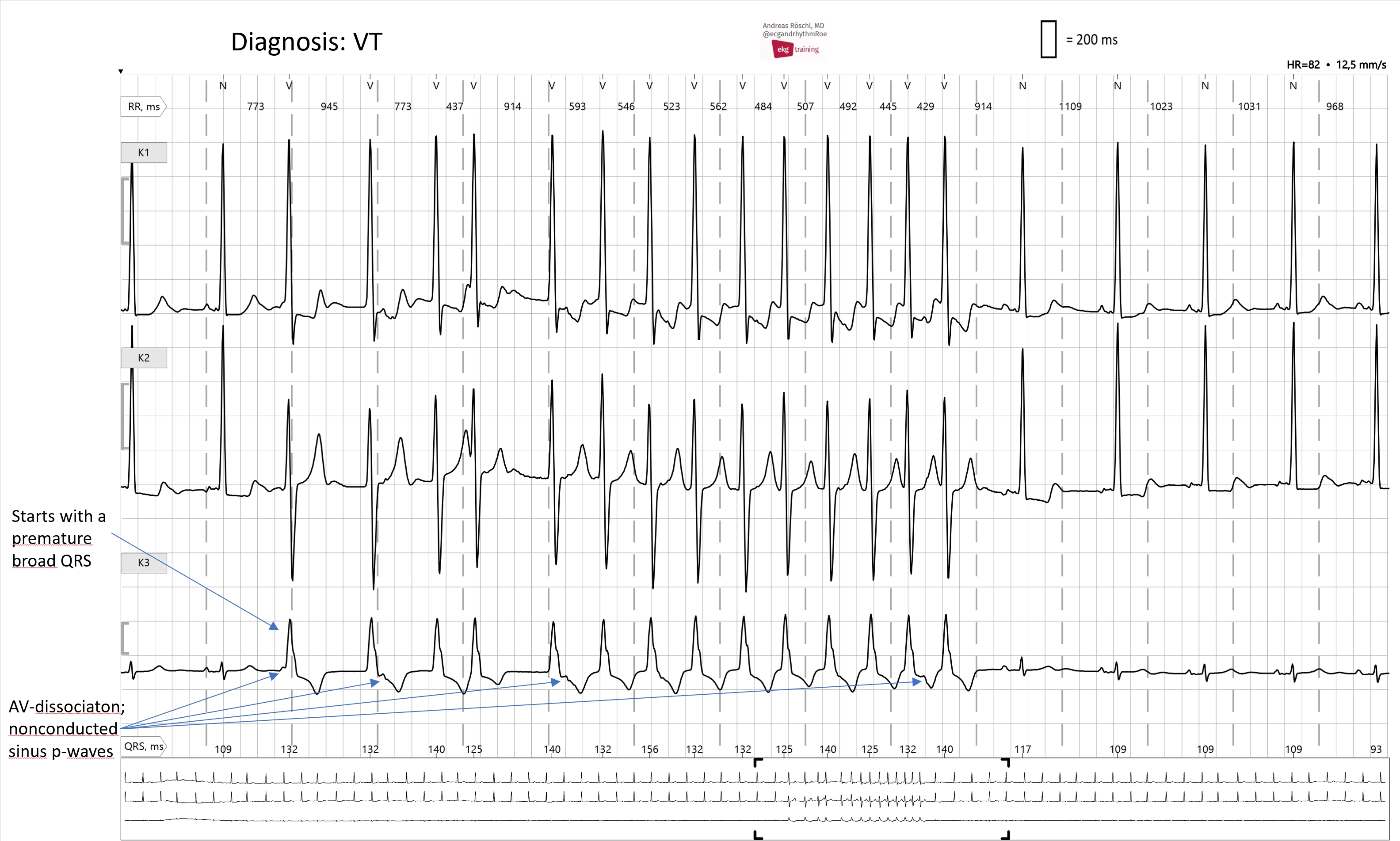
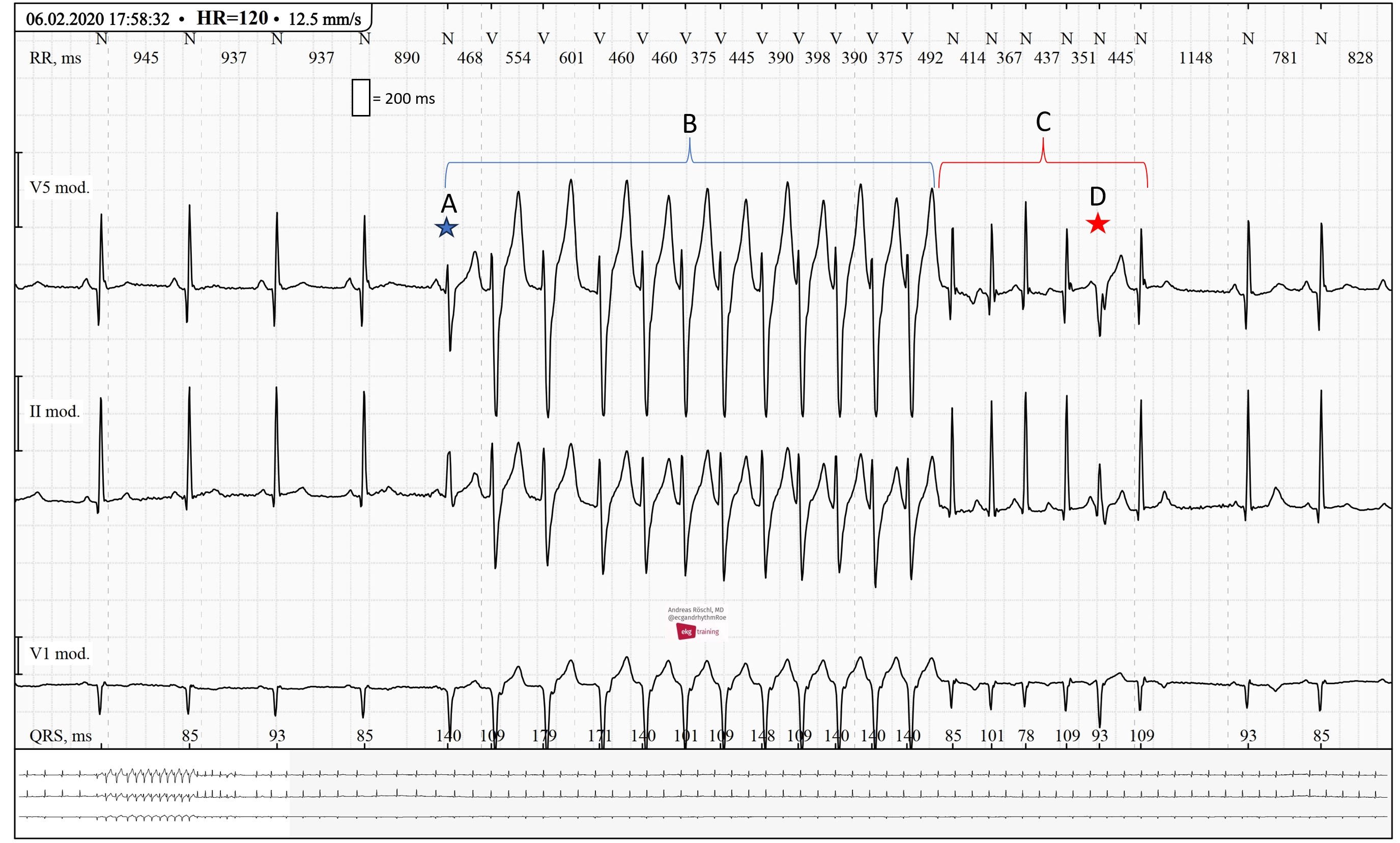
Unfortunately, we do not see capture beats or fusion beats, which would secure the diagnosis of VT. Disassociated P waves would also be a sure sign of VT, but the artifact in this ECG makes it impossible to say whether there are P waves.