
Submitted by Dr A Röschl on Mon, 12/18/2023 - 11:14
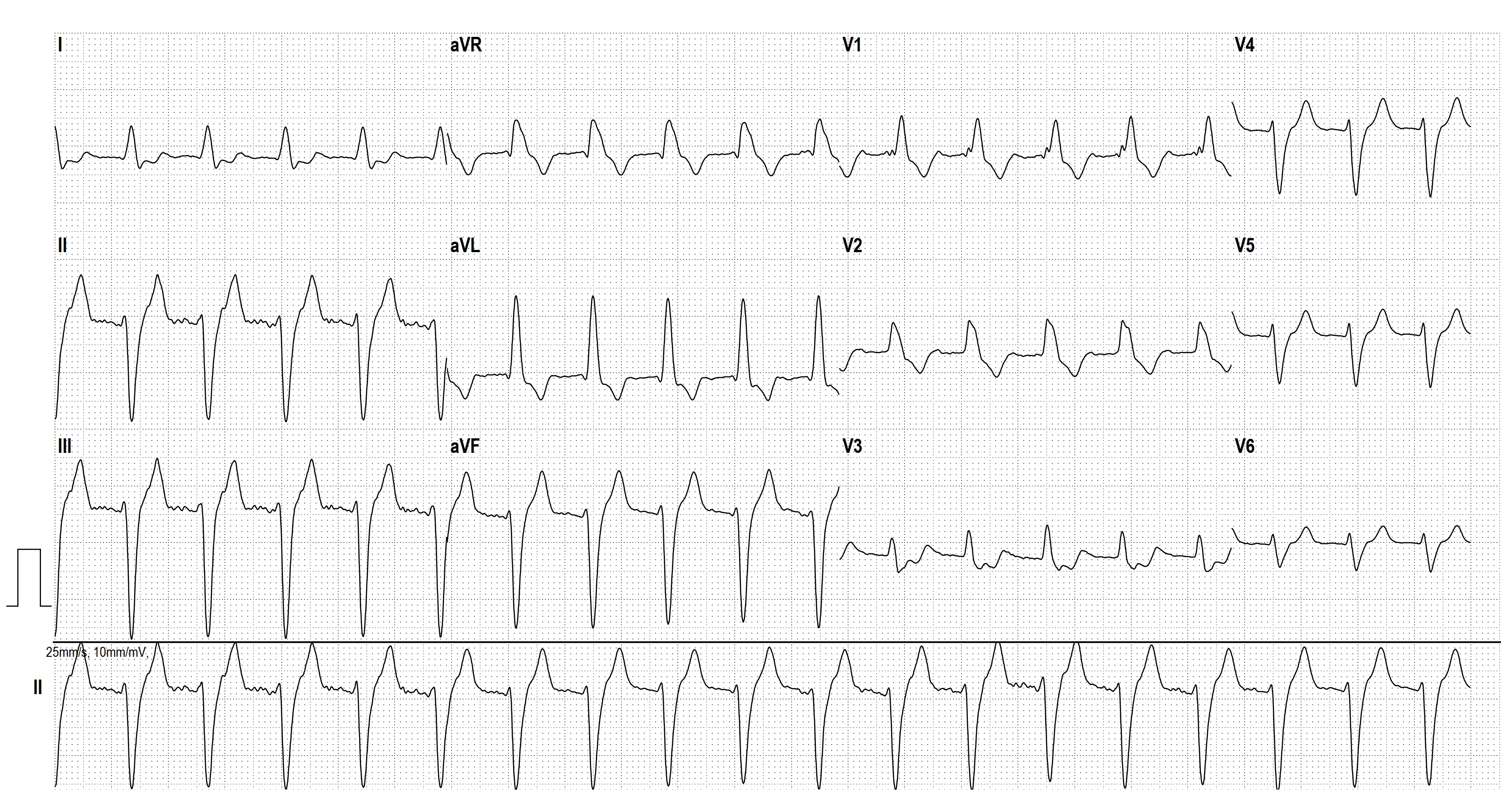
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. 80%, in patients with a previous myocardial infarction (...) approx. 90%). Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. In this constellation, 3 causes must be considered:
1. fascicular tachycardia from the left posterior fascicle of the left tawara fascicle (QRS width usually only around 130 ms, but sometimes significantly longer).
2. AT/AFL with 2:1 conduction in the case of pre-existing bifascicular block
3. AT/ AFL with 2:1 conduction in the case of functional bifascicular block (i.e. first generated by the tachycardia)
In this ECG, it is very difficult to recognize atrial activity. After electrical cardioversion of the existing atrial flutter with 2:1 conduction in this case, this patient showed a picture of SR with RBBB + LAFB.
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.