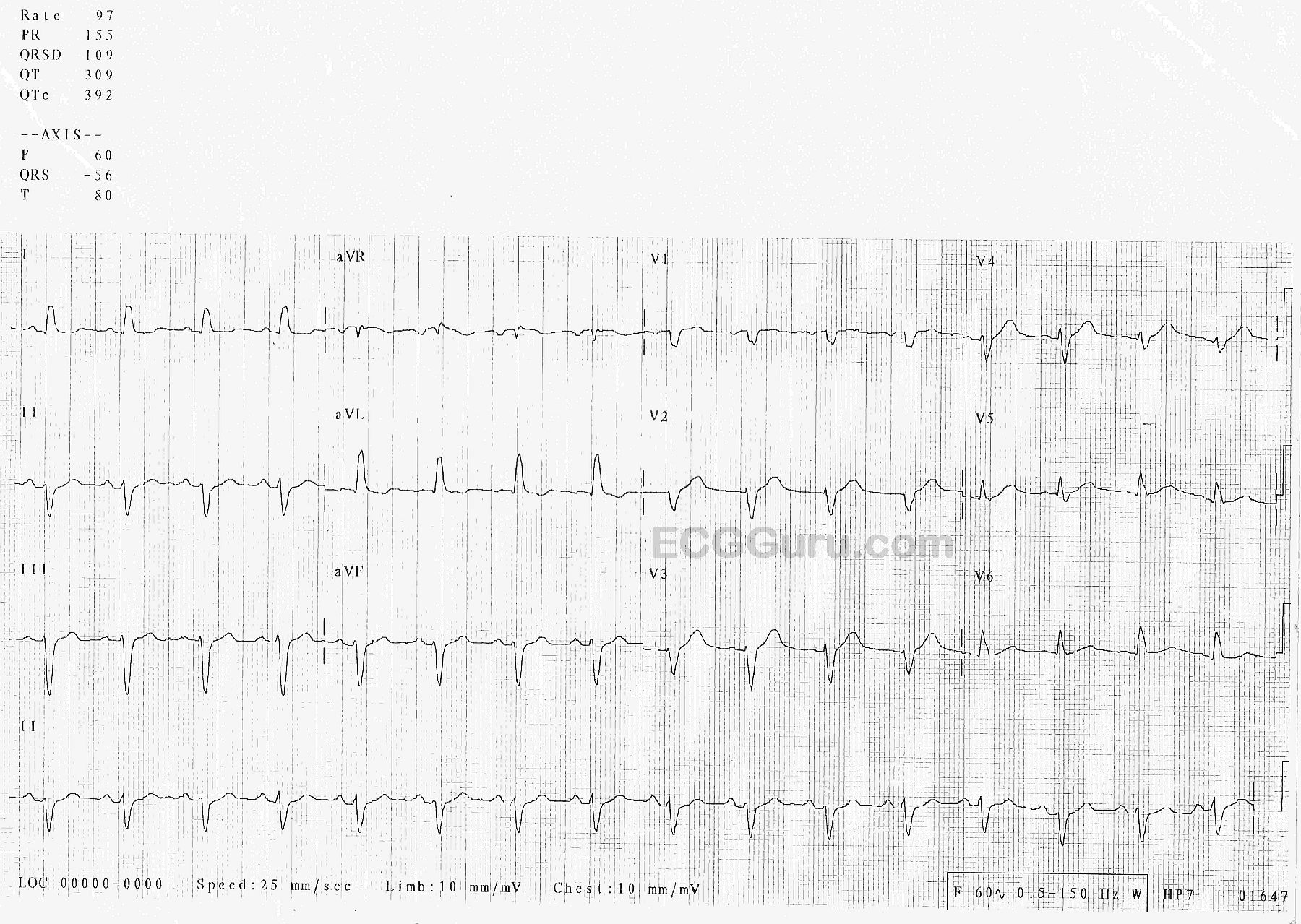
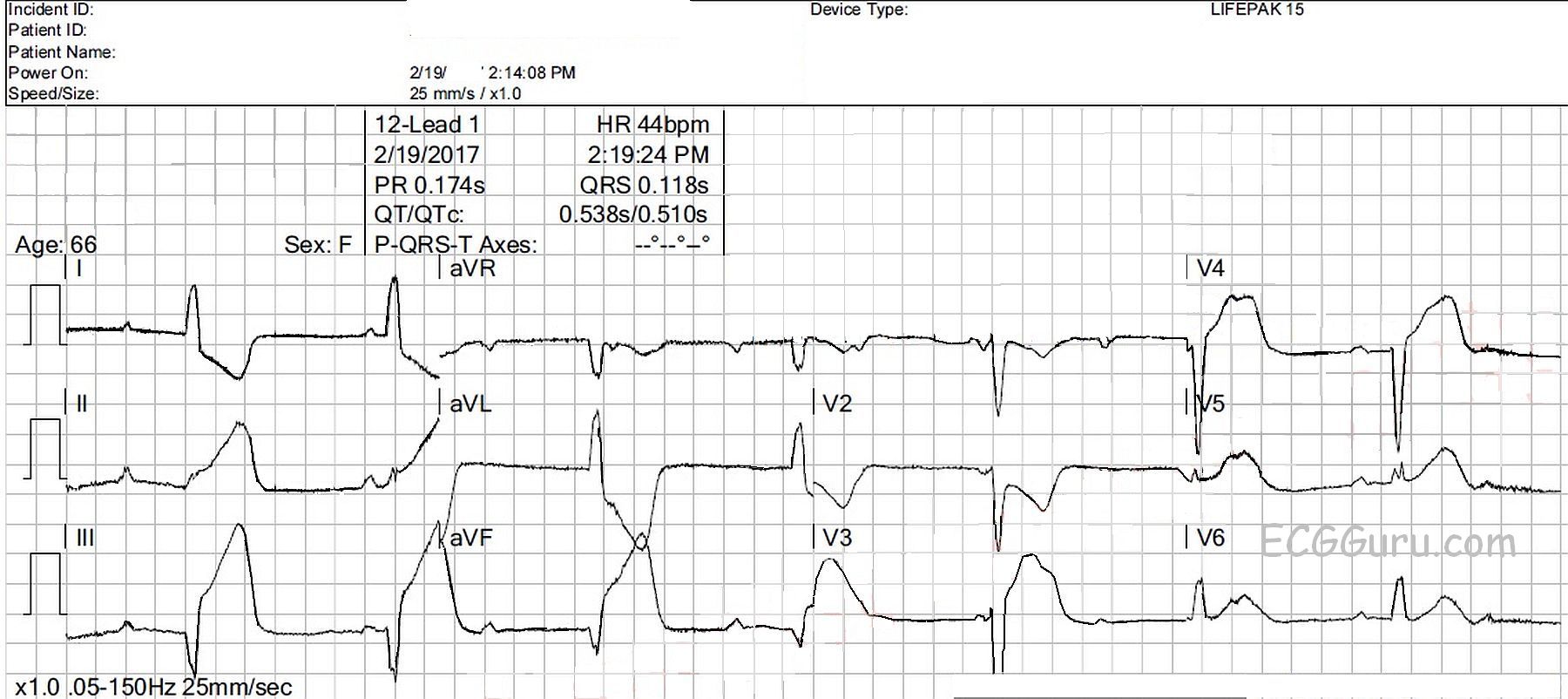
This ECG is from a 66-year-old woman who called 911 for a complaint of chest pain for the past four hours. She also complained of nausea, vomiting, and diarrhea for that time. She was pale and diaphoretic, and her BP was 77/43 sitting up, improving to 90/54 reclining. She denied “cardiac” history. Her medications included: aspirin, an SSRI, cilostazol, amlodipine, umeclidinium and vilanterol inhaler, atorvastatin, levothyroid, and metoprolol. We don’t have a previous ECG. The EMS crew followed their chest pain protocol and delivered the patient to a facility with an interventional cath lab, but they did not designate a “STEMI Alert” because of the wide QRS. It is their protocol to use the term “STEMI Alert” only when no M.I. mimics, such as left bundle branch block, are present.
What does this ECG show? There is an underlying sinus rhythm at 75 bpm. There is AV dissociation, with regular, wide QRS complexes at a rate of 44 bpm. This meets the criteria for complete heart block (third-degree AV block). The morphology of the QRS complexes meets the criteria for left bundle branch block (wide, upright in Leads I and V6, negative in V1). At a rate of 44 bpm, several options for this escape rhythm are possible: 1) junctional escape with LBBB, 2) junctional escape with intraventricular conduction delay due to AMI, and 3) idioventricular escape rhythm. Also, in the presence of IWMI, AV node ischemia is very likely, resulting in AV blocks at the level of the AV node. CHB at the AV node would result in junctional escape rhythm, and CHB below that, in the fascicles of the bundle branches, would result in idioventricular escape. The issue for this patient, and ANY patient, is cardiac output, and we see several reasons for cardiac output to be lower:
· Wide QRS