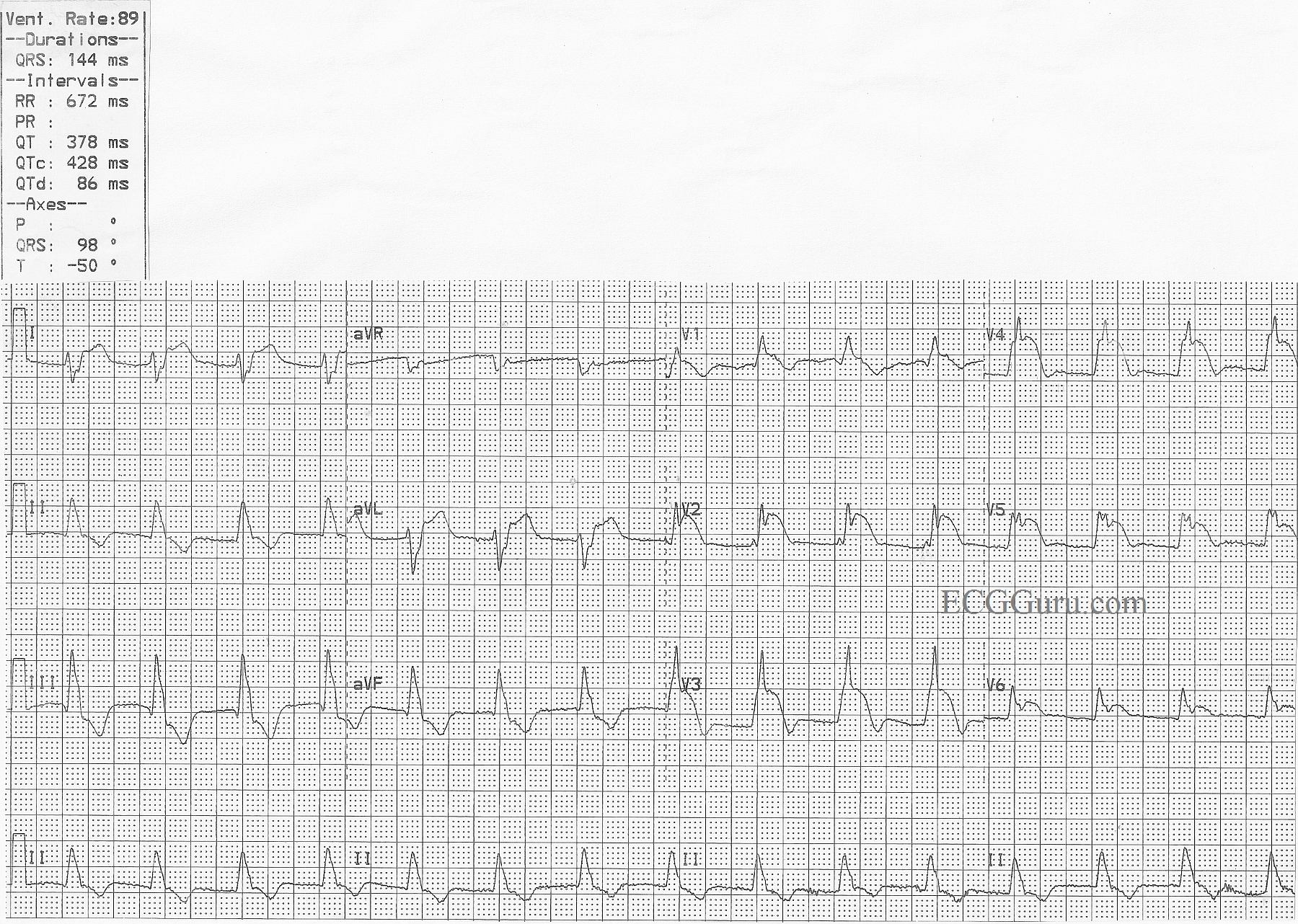
This ECG was obtained from a patient who suffered an occlusion of the left main coronary artery. ST elevation is seen in Leads V1 through V6, as well as I and aVL. This is an indicator that the circumflex artery is included in this M.I., and the occlusion is above the bifurcation of the LM and the circ. The patient also has a right bundle branch block and a left posterior fascicular block. This bi-fascicular block can be a dangerous complication of acute M.I., as two of the three main bundle branches are no longer functional.
The ECG shows typical ST depression, probably reciprocal to the elevation, in the inferior leads.
The right bundle branch block is diagnosed by the following criteria: 1) Wide QRS; 2) Supraventricular rhythm; and 3) rSR' pattern in V1 with Rs with a wide little s wave in Leads I and V6.
The left posterior fascicular block is diagnosed by right axis deviation and by ruling out other causes of right axis deviation. In RAD, Lead III will have a taller positive ( R ) wave than Lead II, and a negative Lead I.
This type of occlusion is often called the "Widow Maker", and requires very rapid intervention to restore blood flow and prevent complicatons. If there is good news, it is that there are no pathological Q waves, which would indicate necrosis, and this patient was taken quickly to a full-service cardiac center with interventional cath labs and open heart surgery available.