If you are an ECG instructor, you probably carefully choose ECGs to illustrate the topic you are teaching. One of the reasons for the existence of the ECG Guru website is our desire to provide lots of such illustrations for you to choose from.
Sometimes, though, an ECG does not clearly illustrate one specific dysrhythmia well, because the interpretation of the ECG depends on so many other factors. In order to get it “right”, we would need to know information about the patient’s history, presentation, lab results, or previous ECGs. We might need to see the ECG done immediately before or after the one we are looking at. Some ECG findings must ultimately be confirmed by an electrophysiology study before we can know for sure what is going on.
For those of us who are “ECG nerds”, it can be fun to debate our opinions and even more fun to hear from wiser, more advanced practitioners about their interpretations.
My belief, as a clinical instructor, is that we must teach strategies for treating the patient who has a “controversial” ECG that take into account the level of the practitioner, the care setting, and the patient’s hemodynamic status. In some settings, it might be absolutely forbidden for a first-responder to cardiovert atrial fibrillation, for example. But atrial fib is routinely cardioverted under controlled conditions in hospitals. The general rule followed by emergency providers that “all wide-complex tachycardias are v tach until proven otherwise” has no doubt prevented deaths in situations where care providers did not agree on the origin of the tachycardia.
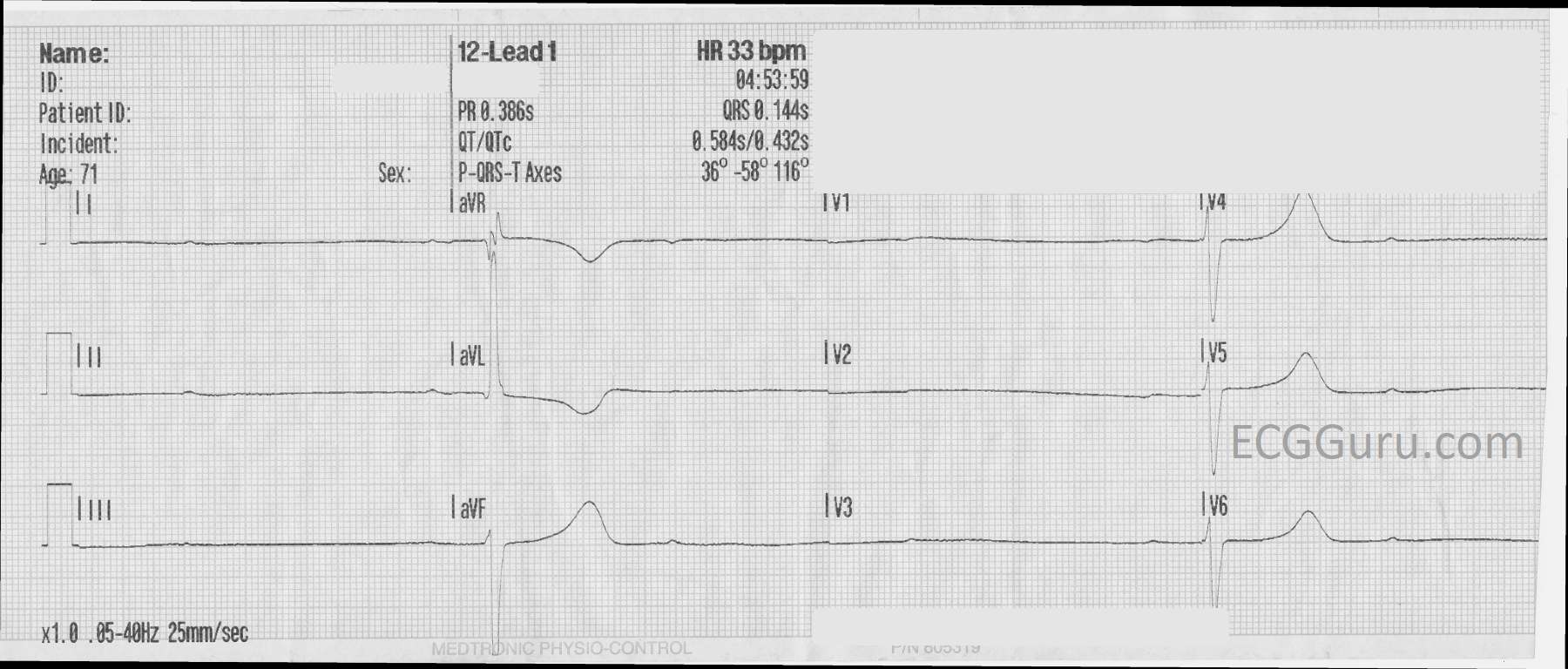
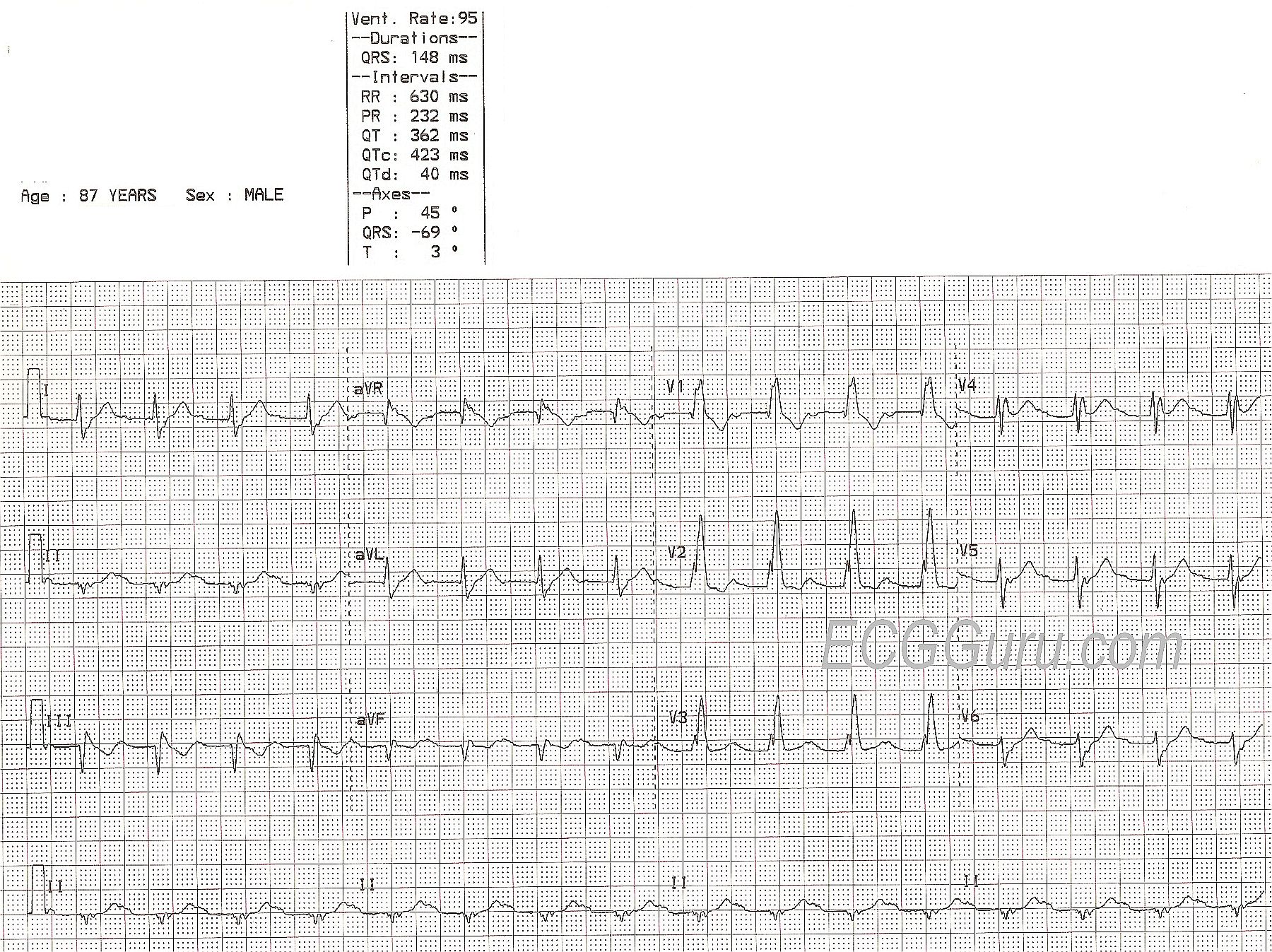
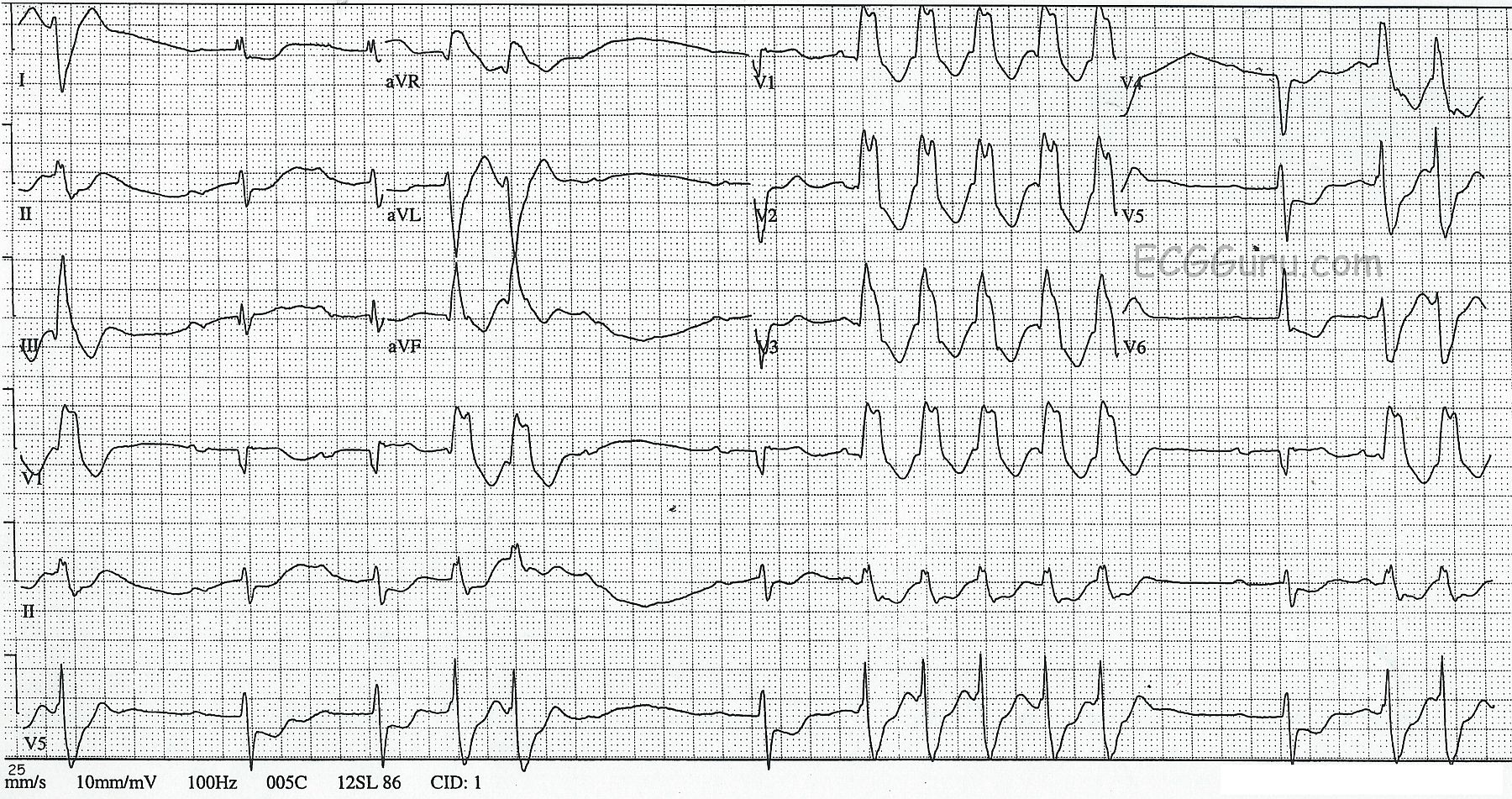
The ECG: We do not have much patient information to go with this ECG, just that it is from a 71-year-old woman who developed severe hypotension and lost consciousness, but was revived with transcutaneous pacing. Here is what we do know about this ECG:
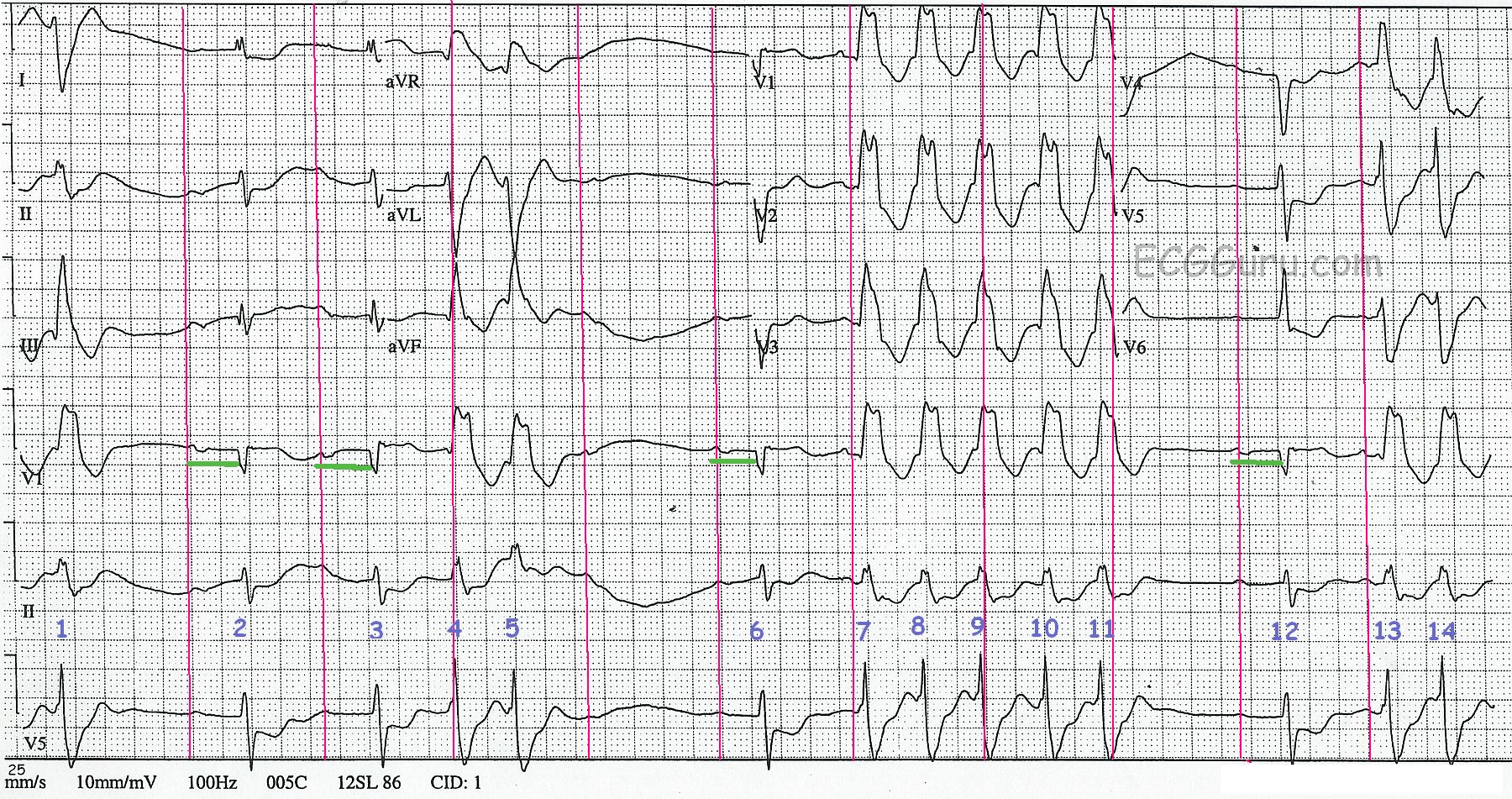
· There are regular P waves, at a rate of about 39 bpm (sinus bradycardia).