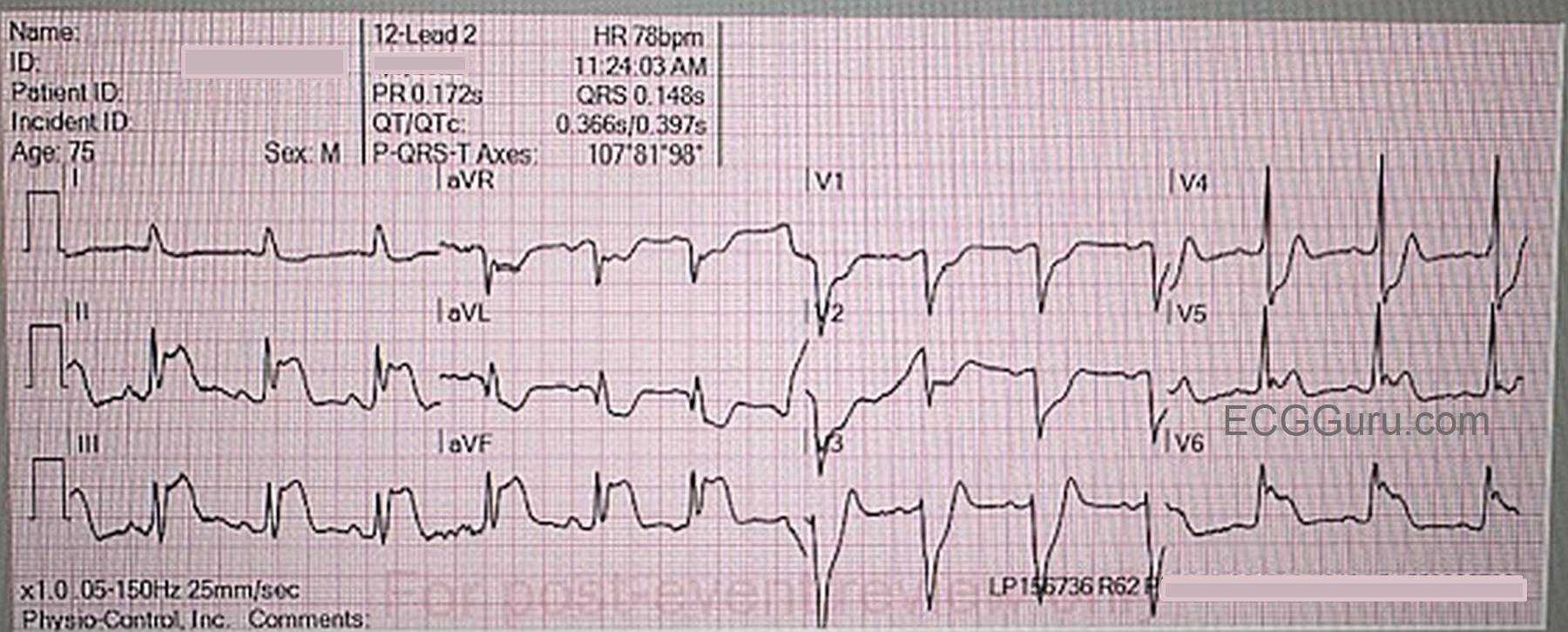
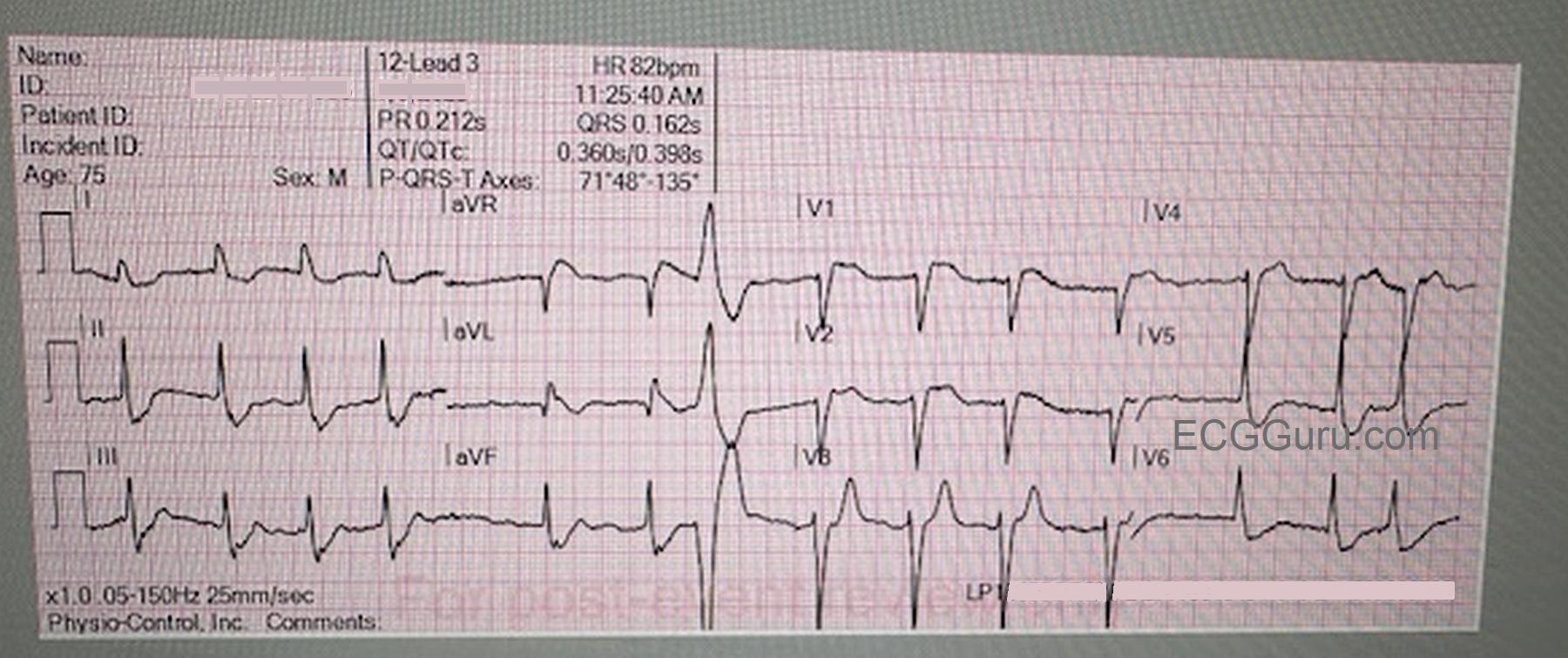
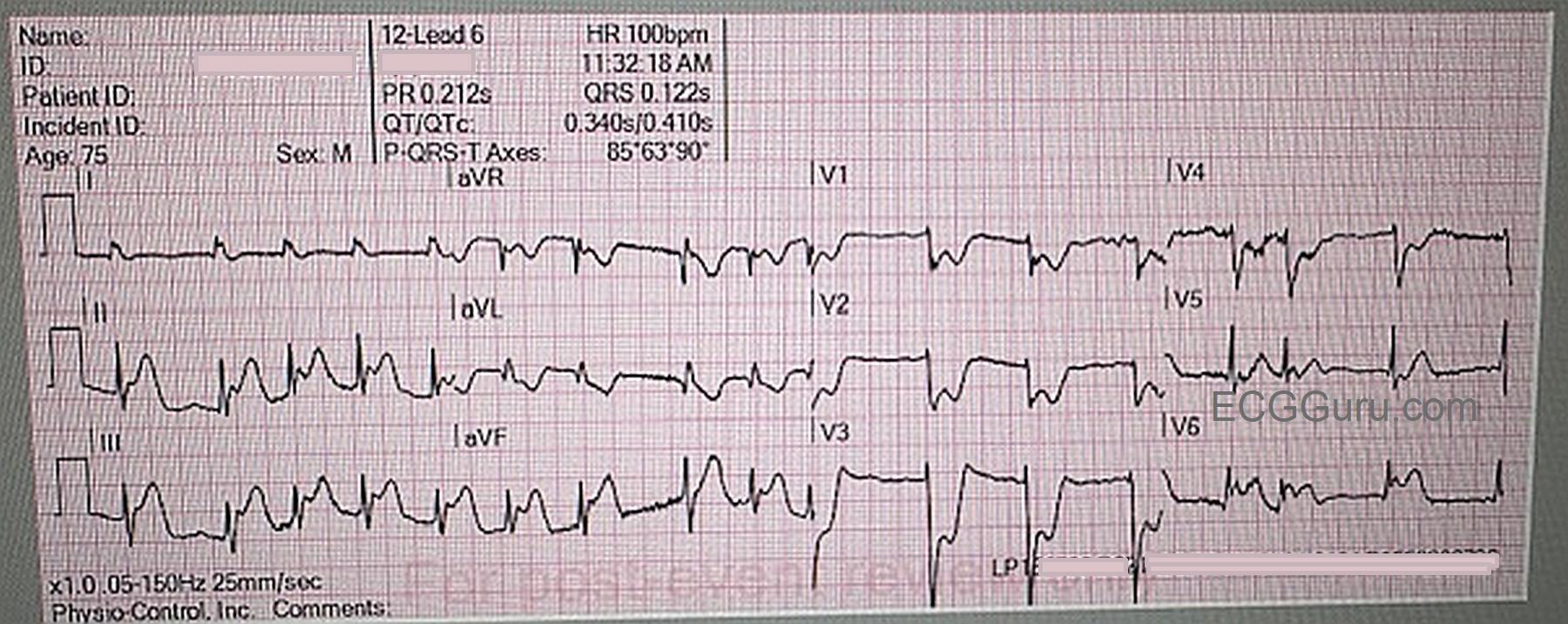
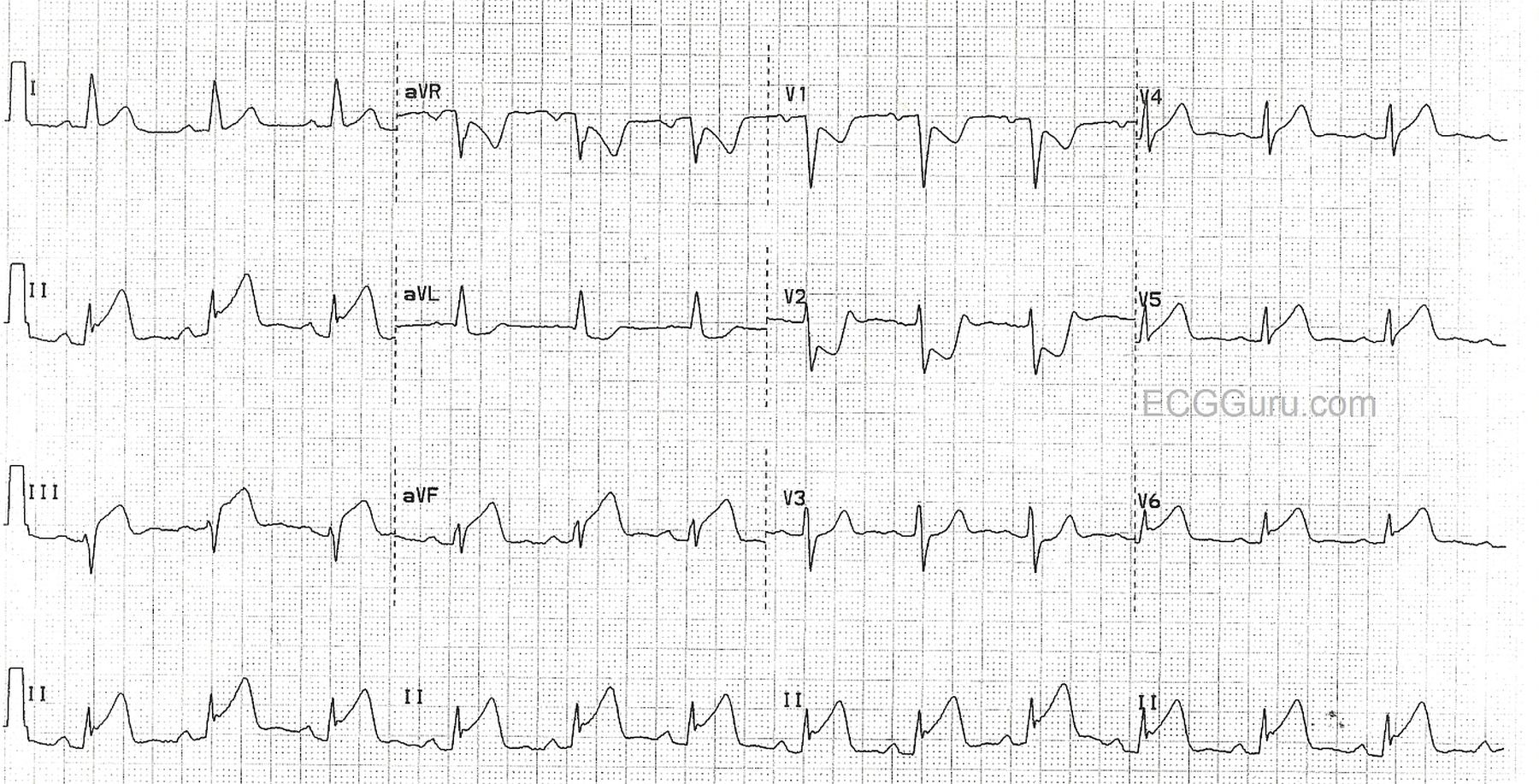
This ECG and rhythm strip are from a 78 year old man with chest pain, but we have no other clinical data. This is a good example of inferior and low lateral injury, demonstrating the large amount of heart muscle that can be damaged when a dominant RCA or circumflex artery is occluded. The low lateral wall is often included in an inferior wall M.I. when the RCA wraps around the left side of the heart, or the circumflex perfuses the posterior descendng artery and the inferior wall.
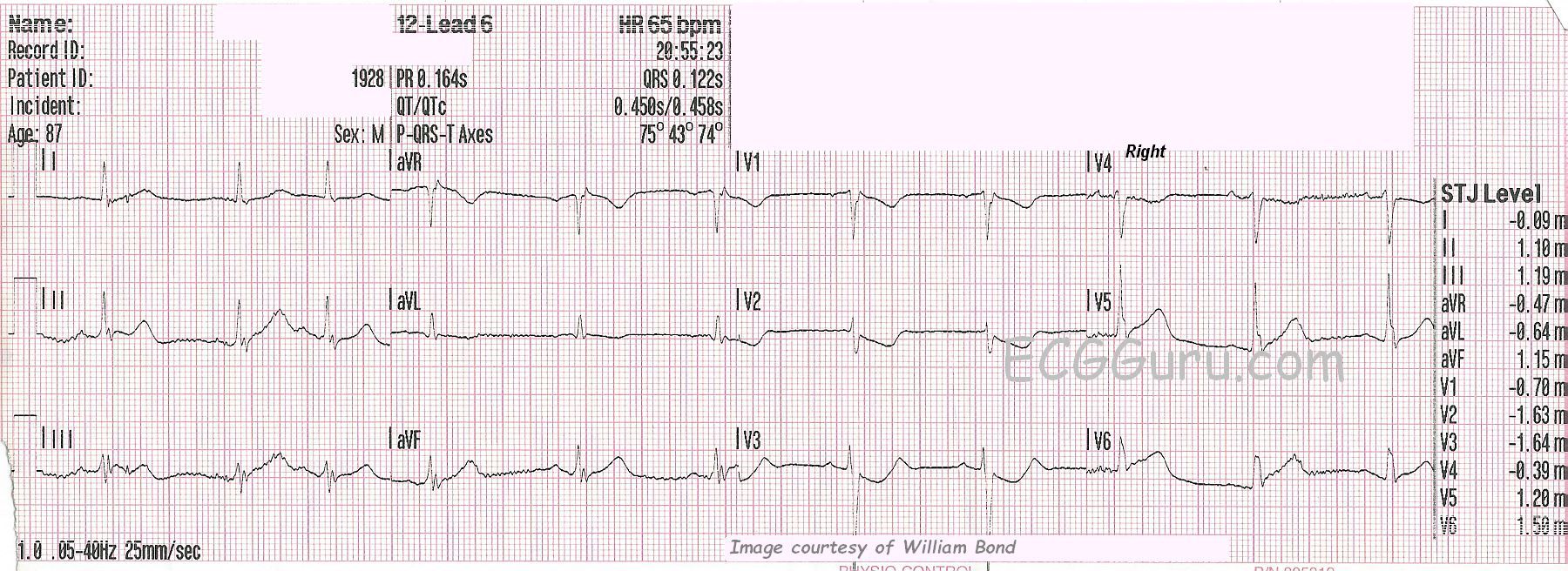
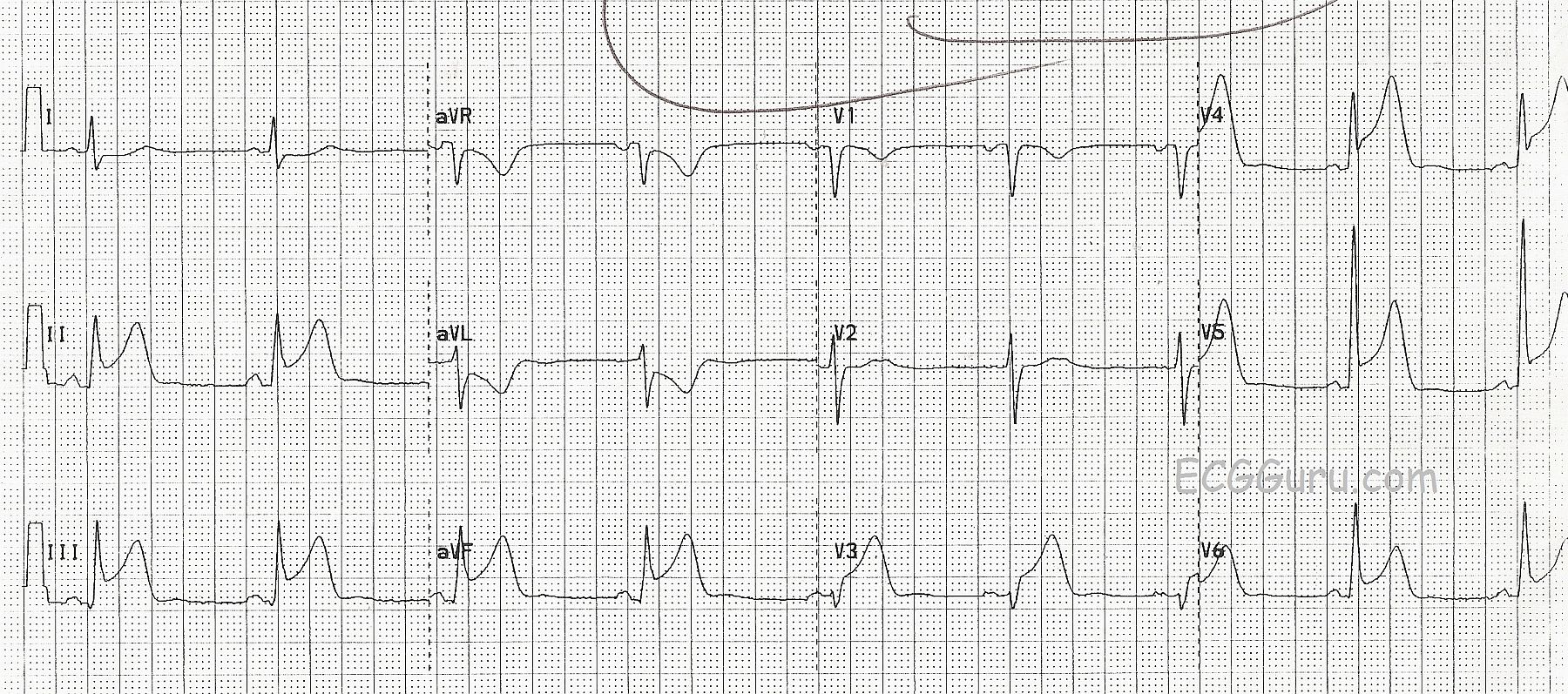
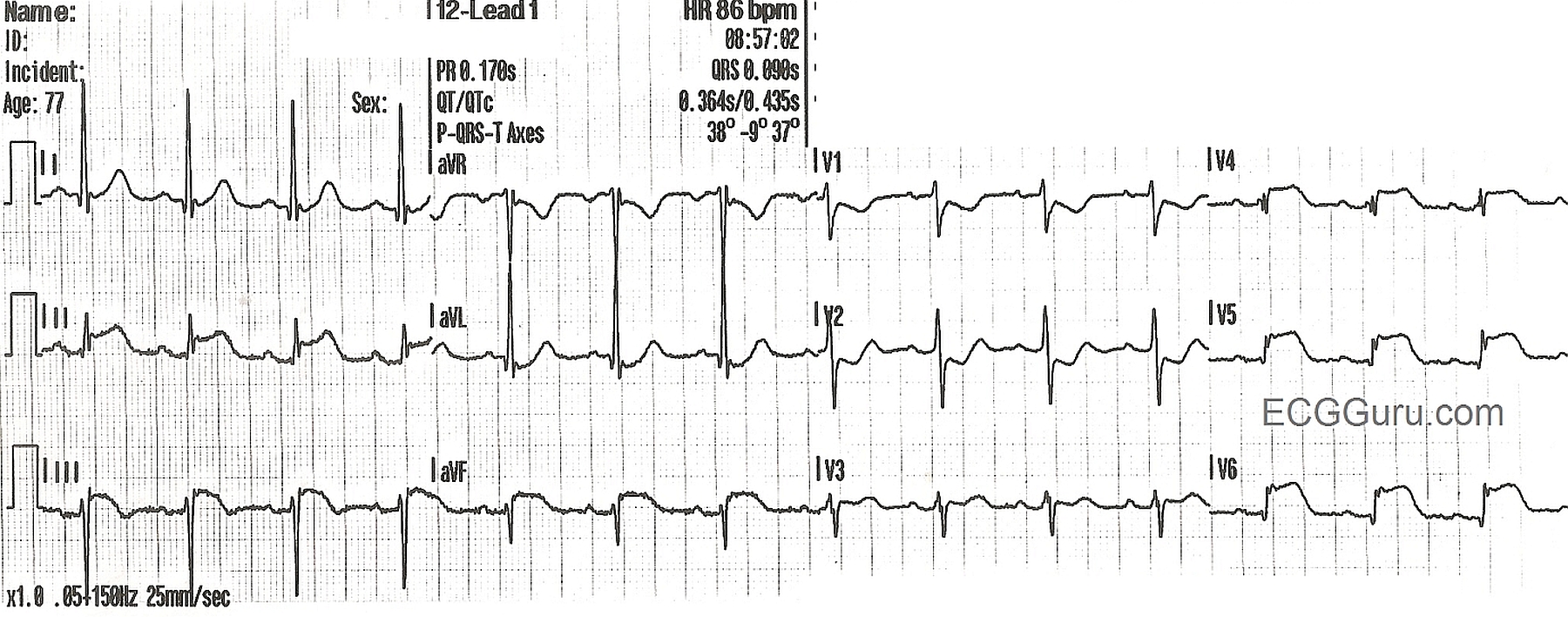
In this ECG, we see a sinus rhythm with obvious ST segment elevation in Leads II, III, and aVF, with reciprocal ST depression n Lead aVL. There is reciprocal ST depression in V1 and V2, indicating that the inferior wall injury extends up the posterior wall until it is seen by the anterior leads V1 and V2 as ST depression. The term "posterior wall" has come into some scrutiny recently, but it is still commonly used, so we use it here. There is also ST elevation in Leads V4, V5, and V6, reflecting the low lateral wall.
This is a great example of how the SHAPE of the ST segment is often altered in acute M.I. as well. Leads II, V4, V5, and V6 have obvious "flattening" of the ST segment. Even when the ST elevation is minimal, this shape is a STRONG indicator of M.I. Lead III has a convex-upward shape, another giveaway for an M.I. diagnosis.
Adding to the evidence for a diagnosis of acute M.I. are the associated signs: T wave inversion in Lead III (a sign of ischemia), and poor R wave progression in V3 through V6. Since V3, V4, V5, and V6 should all have strong R waves, this could be an ominous sign of impending pathological Q waves, a sign of myocardial necrosis.
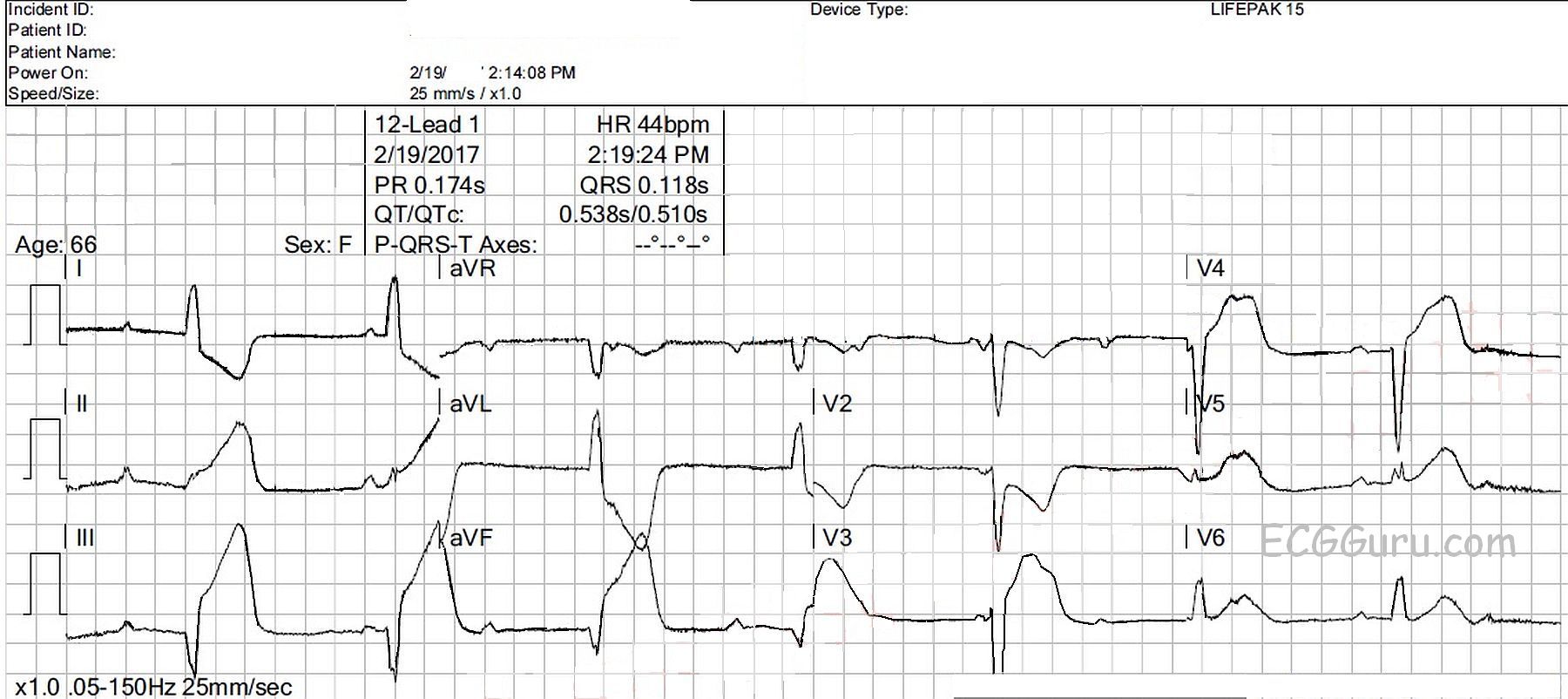
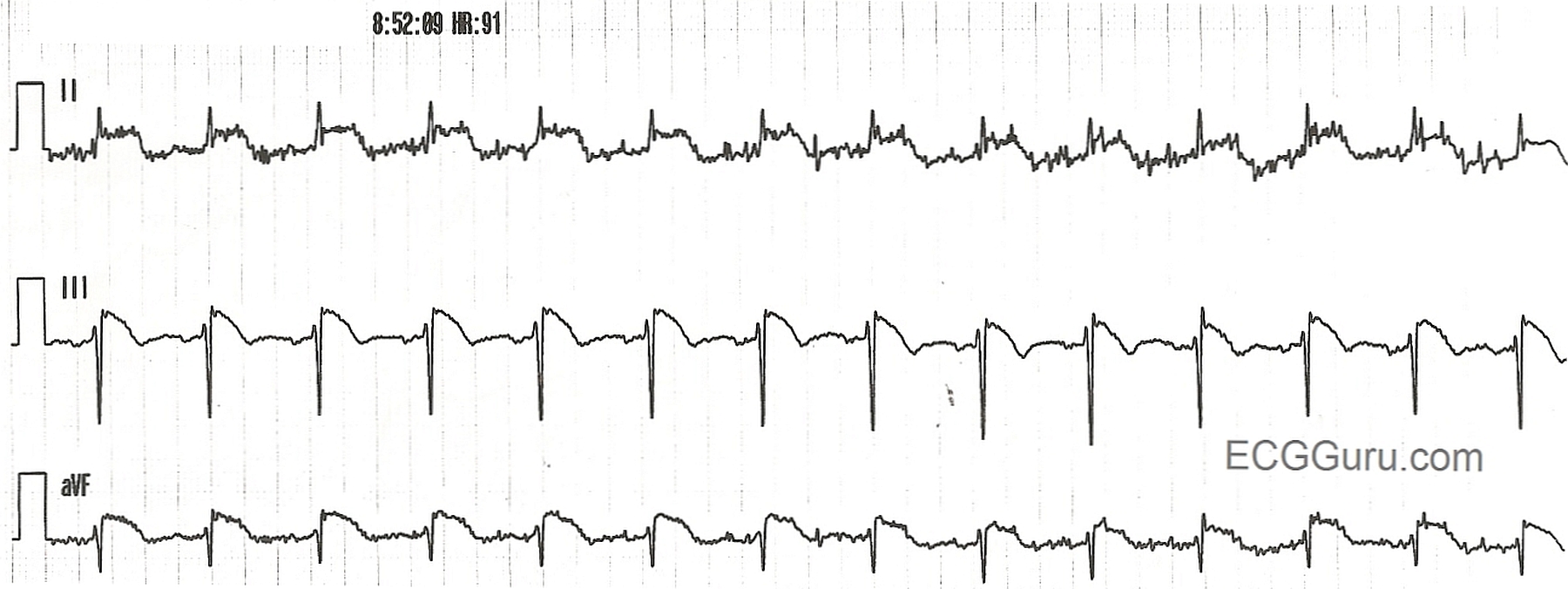
The rhythm strips in this case demonstrate ST elevation also. There is artifact in Leads II and aVF. This example can be used for beginners who are learning lead concepts. Ask, "Which limb is the artifact coming from?" The answer is the right arm, because Lead III doesn't use the right arm, and it is clear of artifact.