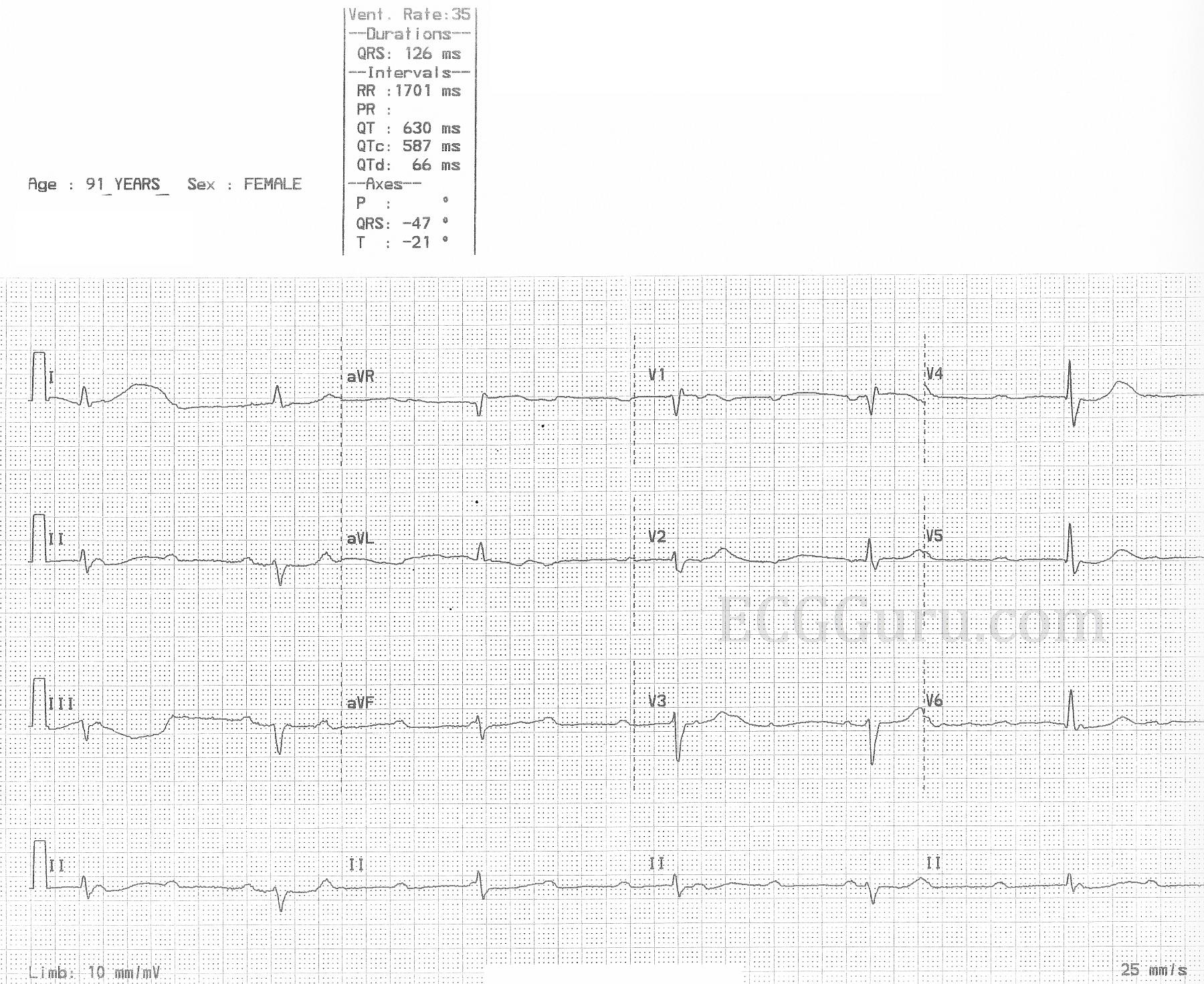
The patient: This ECG was obtained from a 91-year-old woman who was complaining of weakness. Unfortunately, we have no other information.
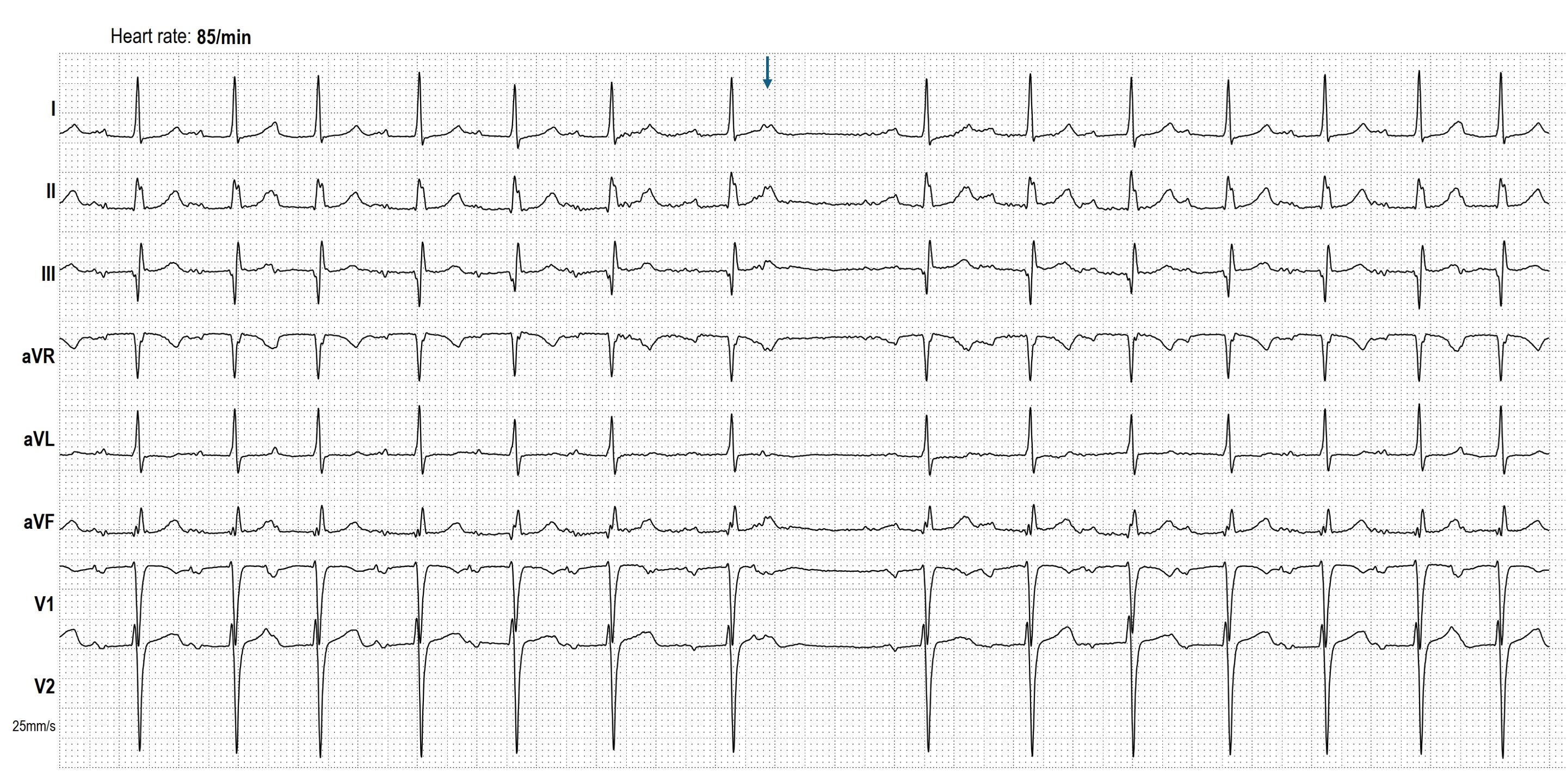
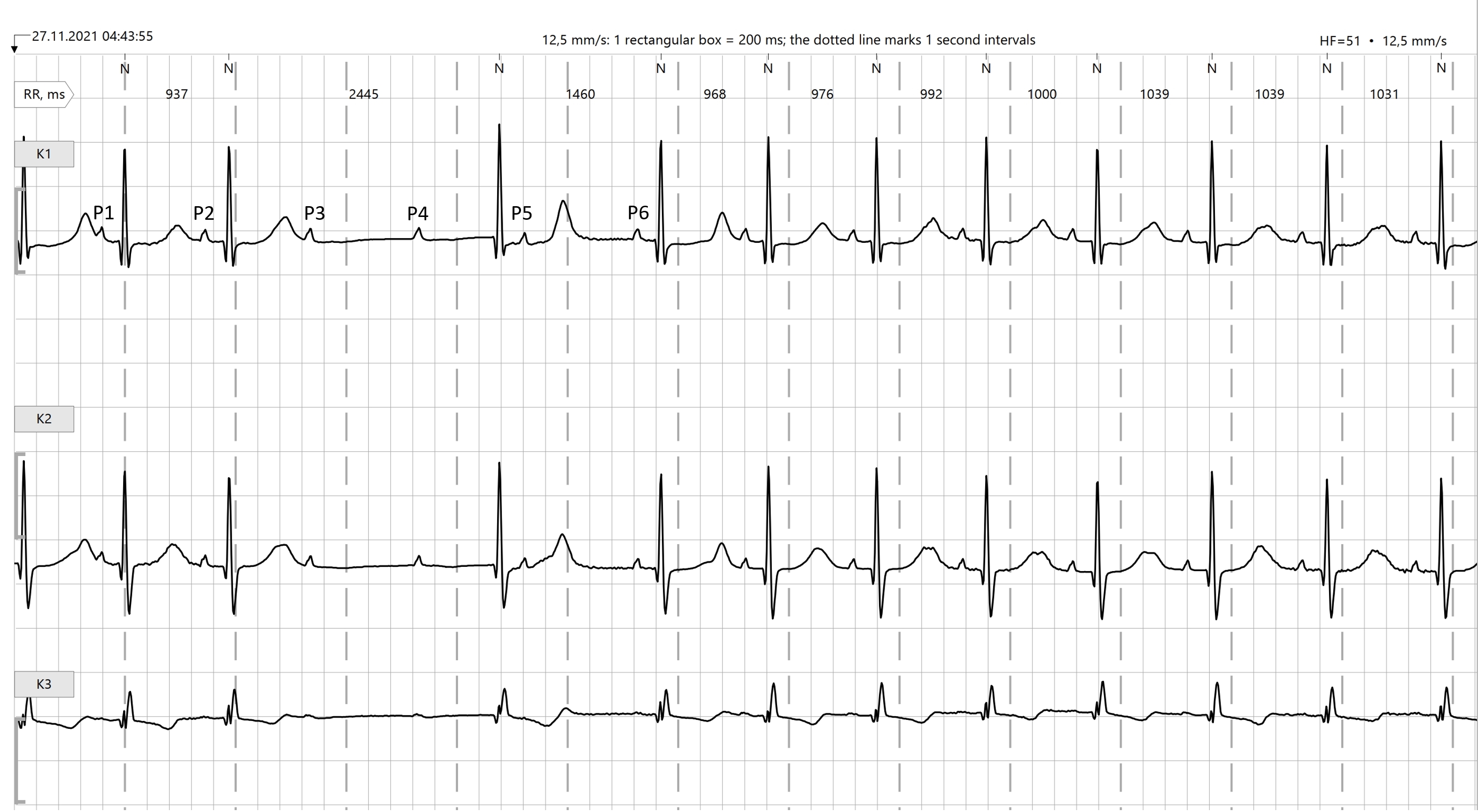
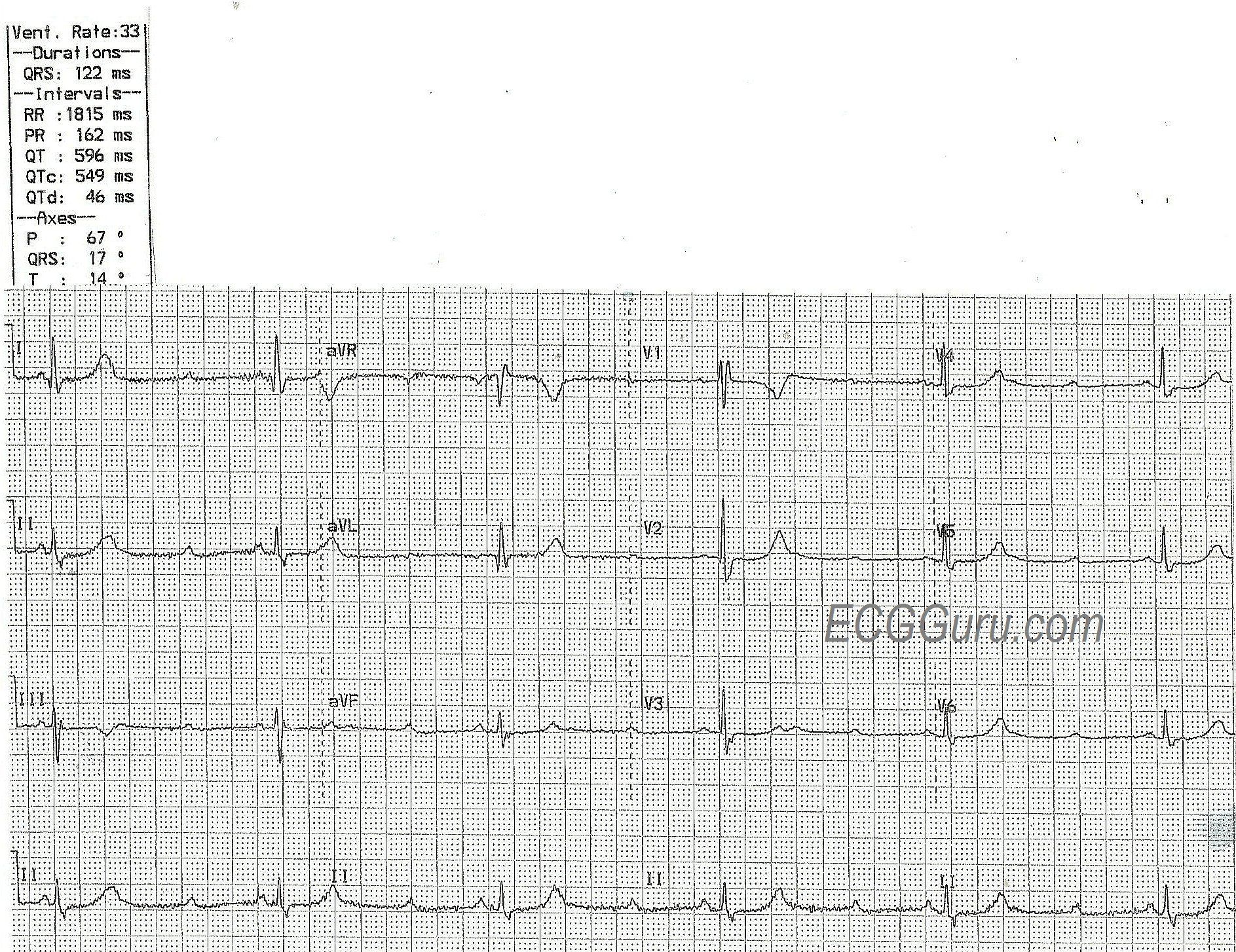
The ECG: This ECG has something for your basic students, and even more for the more advanced learners. The first thing that anyone should notice is the slow rate. The ventricular rate is around 35 bpm, and regular. If the patient is showing signs of poor perfusion, we would stop here and prepare to increase the rate with a temporary pacemaker (transvenous or transcutaneous). Why is the rate so slow? There is no P wave in front of each QRS, so this is not sinus bradycardia. Rather, we see P waves at a rate of approximately 100 bpm, wit a very regular rhythm. Beginners should “march out” the P waves with calipers or by marking a straight edge piece of paper. There are 15 P waves on this ECG – some are buried within QRS complexes (QRS #3) or T waves (QRS #4).
Because there are two distinct, regular rhythms, but they do not track with one another, we know this is possibly third-degree AV block (complete heart block). Another clue is that there are no steady, repetitive PR intervals, which means there is no relationship between the atrial rhythm and the ventricular rhythm.
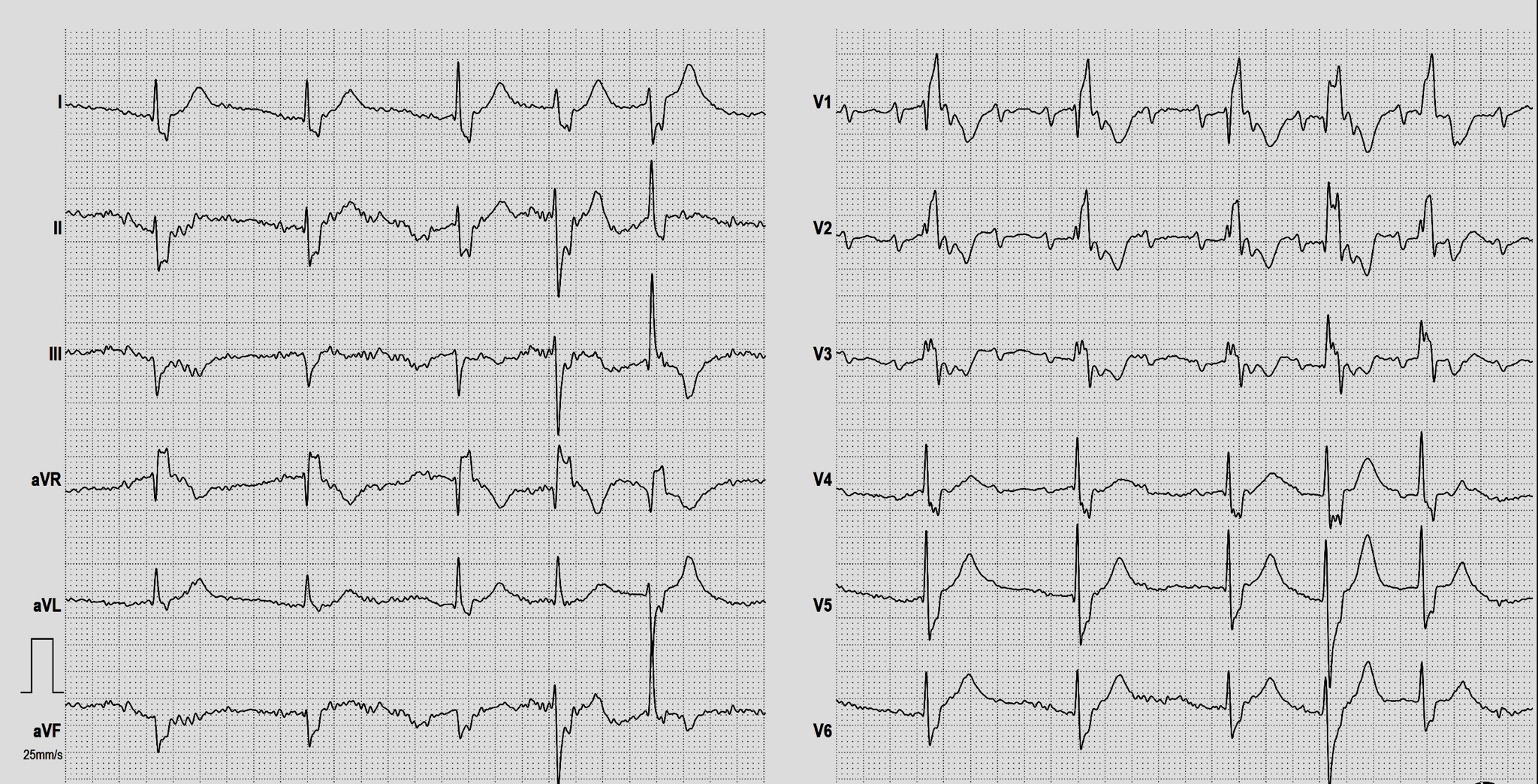
For more advanced learners, it is helpful to try to identify the origin of the escape rhythm. If it is junctional, the AV block is above the junction. If the escape is ventricular, the AV block is below the junction. A junctional rhythm is usually between 40 – 60 bpm, with a narrow QRS. Ventricular escape rhythms are usually less than 40 bpm and with wide QRS complexes. This ECG will be a little challenging on this front, because the rhythm has some characteristics of junctional rhythm and of ventricular rhythm.