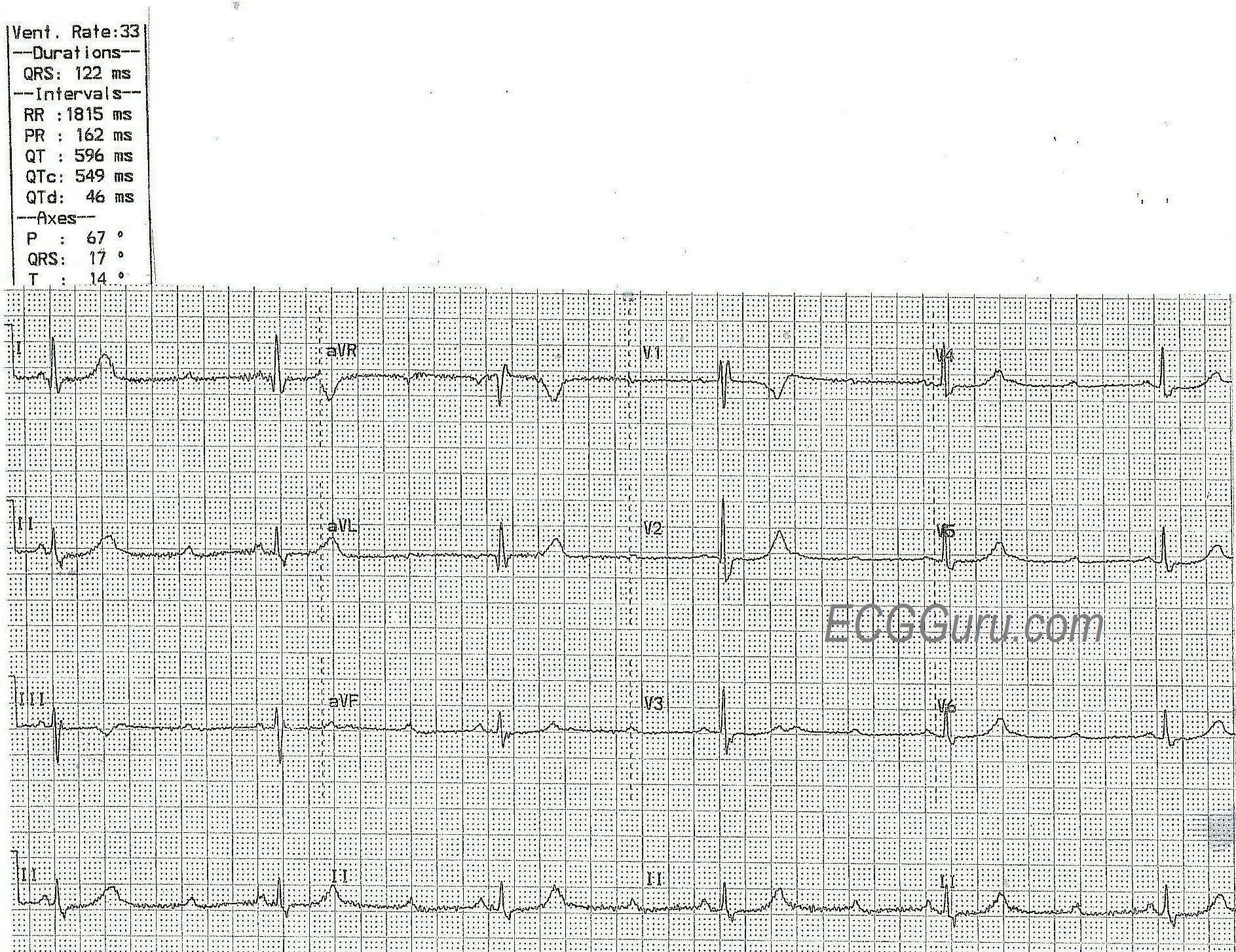
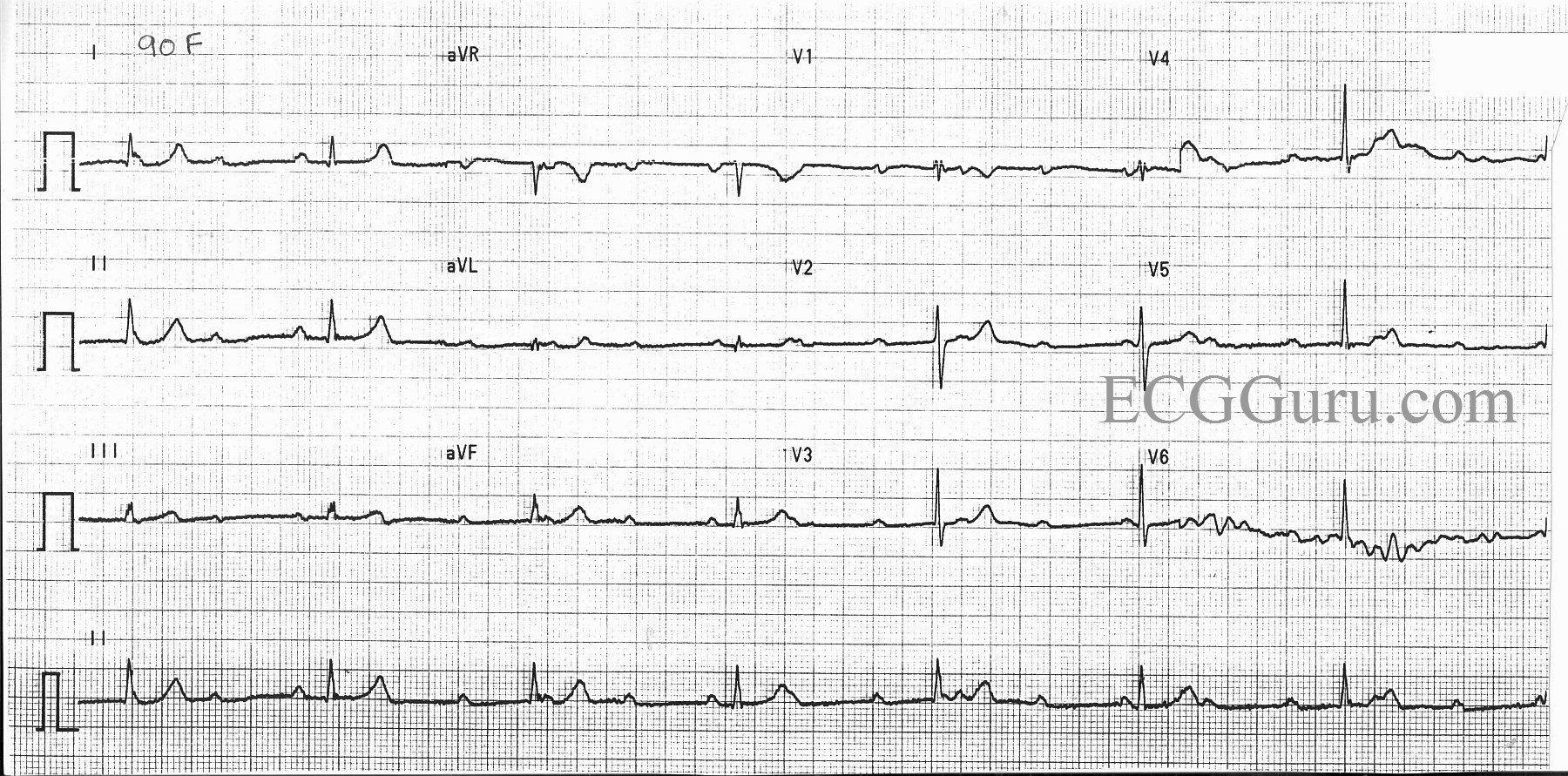
This ECG was taken from a 90-year-old woman. We have no other history, unfortunately. It is a good example of a sinus rhythm with complete AV block, also called third-degree AV block.
The defining characteristics of this rhythm include: 1) an underlying rhythm that is regular and with a physiological rate. In other words, the P waves are not so fast that they would not be expected to conduct one-to-one. 2) a second rhythm of regular QRS complexes that is unrelated to the P waves.
Occasionally, a P wave may occur before a QRS and appear to have a PR interval. This is just a chance meeting, as both rhythms (P waves and QRS complexes) are regular AT DIFFERENT RATES, so we would expect them to occur near each other from time to time. NONE of the P waves are being conducted to the ventricles to produce QRS complexes. This is a good ECG to demonstrate "marching out" the P waves to see that they are very regular, even though some are hidden in the QRS, ST segment, or T waves.
In this case, the "escape rhythm" occurs from the AV junction. The AV junctional pacemakers are "set" at a rate of about 40 - 60 beats per minute. Normally, the sinus rhythm arrives in the AV junction faster than that, depolarizing the junctional pacemakers and preventing them from firing spontaneously. In complete AV block, the atrial impulse never arrives, so the junctional pacemaker is free to "escape" and become the primary pacemaker of the heart. We recognize this rhythm as junctional because the QRS complexes are narrow, and the rate is around 40 bpm. Knowing that the escape rhythm is from the junction tells us that the AV block is in the AV node. The AV junction is the first available pacemaker below the block. Had the complete AV block been lower, in the bundle branches, the QRS would have come from the ventricles and would have been wide and slower.
In very general terms, this "supra-Hisian" type of AV block is preferable to a "sub-Hisian" block. The rate is faster, and the QRS complexes narrow, both conditions causing a better cardiac output than wide QRS complexes and extremely slow rates. However, the effect of the block on the patient has a lot to do with the cause of the block and the symptoms the slow rate cause. Emergency treatment of the rate may be necessary if it causes a drop in blood pressure and perfusion. Some patients with this type of block will need a permanent implanted pacemaker, but not all.