
Submitted by Dr A Röschl on Sat, 06/03/2023 - 04:32
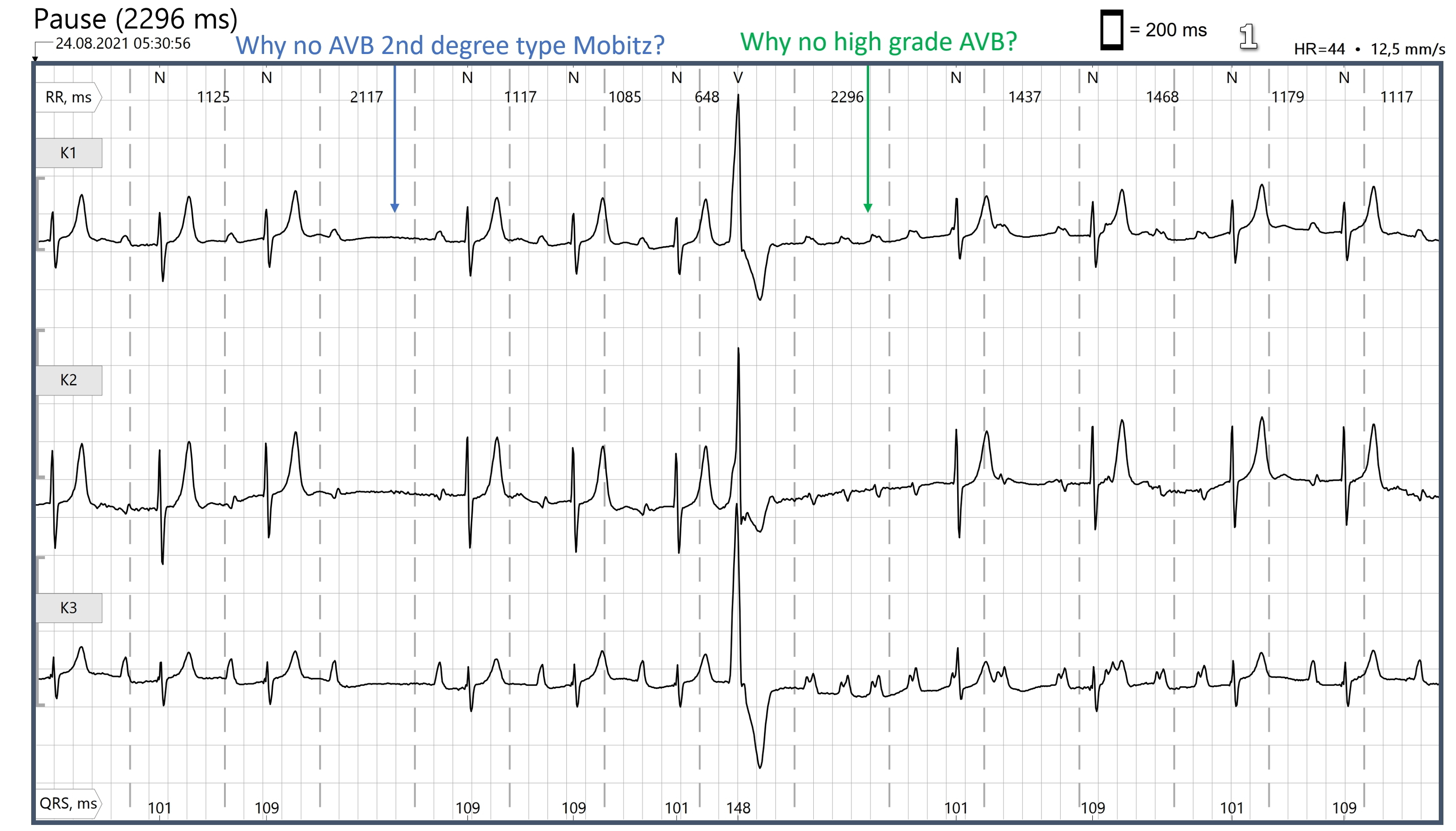
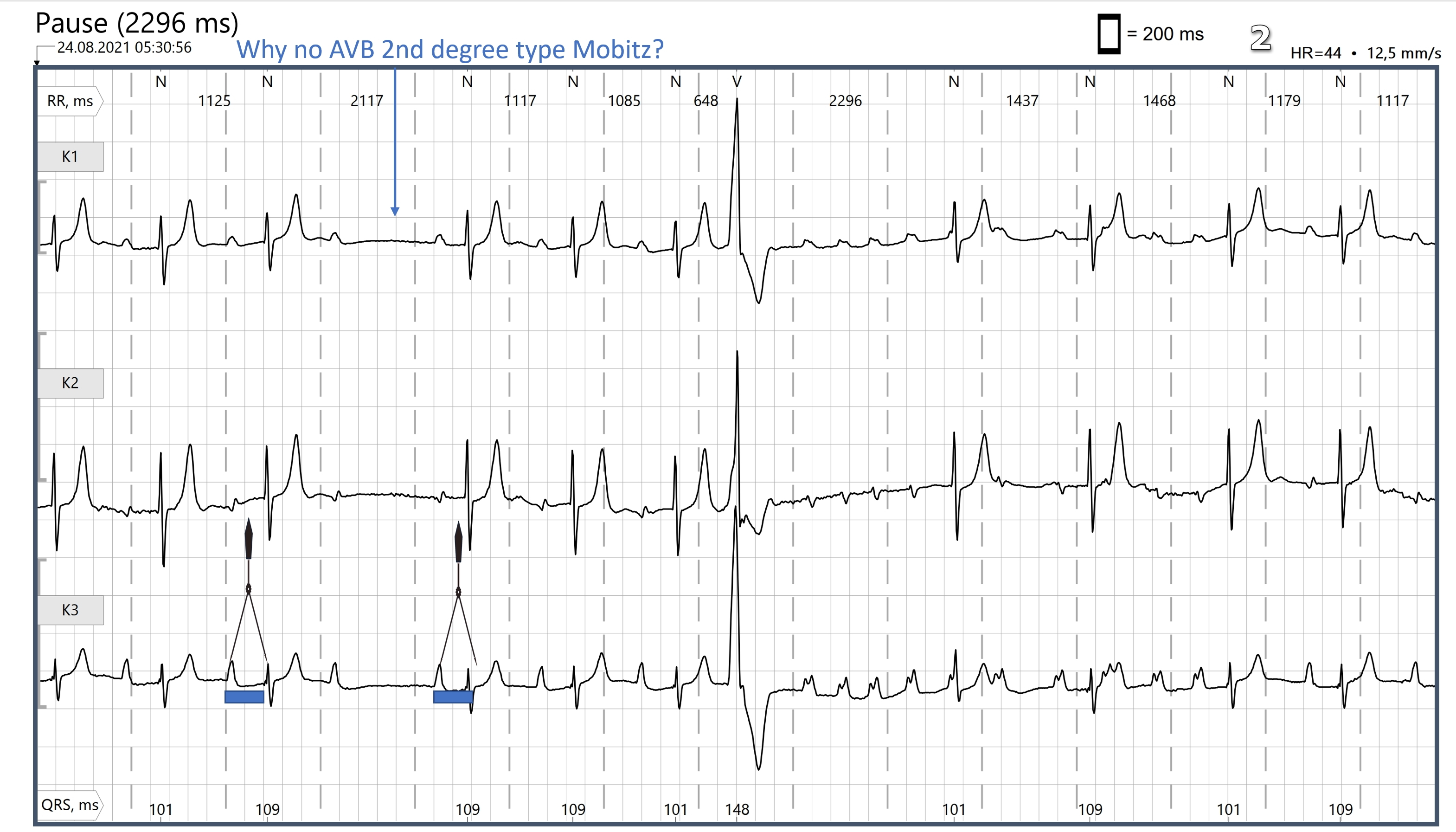

(Image 1) Why is there no second-degree AVB Mobitz type II and no high-grade AV block? To the first question: Basically, second-degree AV block Mobitz type II is rare. The two ECG patterns that can easily be confused with Type II Mobitz block are: blocked/non-conducted PACs and second-degree AVB Mobitz type I (Wenckebach). (Image 2) You have to compare the PR duration before the pause and after it. With the naked eye, the difference is often difficult to recognize, a pair of calipers does a good job here. In this ECG, the PR duration after the failed QRS is significantly shorter than that before the pause, so there is a Wenckebach block here. Due to the time of day (5:30 am), it can be assumed that the patient was still asleep. Under influence of the vagal nerve, AVB Wenckebach is common. In most cases there is no need for any treatment. (Image 3 ) 1, 2 and 3 are transmitted P waves (in sinus rhythm) with a significantly prolonged PR interval (first-degree AVB). 4 represents the next P (at the end of the QRS of the PVC) that comes from the sinus node. Due to the refractority period of the AV node or the bundle branches, this sinus beat can not be conducted to the ventricles. At 5, a high-frequency atrial tachycardia begins with a rate of around 170 bpm. 5 to 7 are not conducted. 8 is conducted, 9 and 10 not conducted, 11 conducted, 12 and 13 not conducted, 14 conducted. Then the tachycardia ends and 15 is the first P wave that comes from the sinus node. Thus, there is no high-grade AV block in the classic sense, because we are dealing here with atrial tachycardia and the AV node is allowed to block high-frequency PAC runs. This is not pathological, but is considered to be a "physiological block".
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.