
Submitted by Dawn on Tue, 07/07/2015 - 15:56
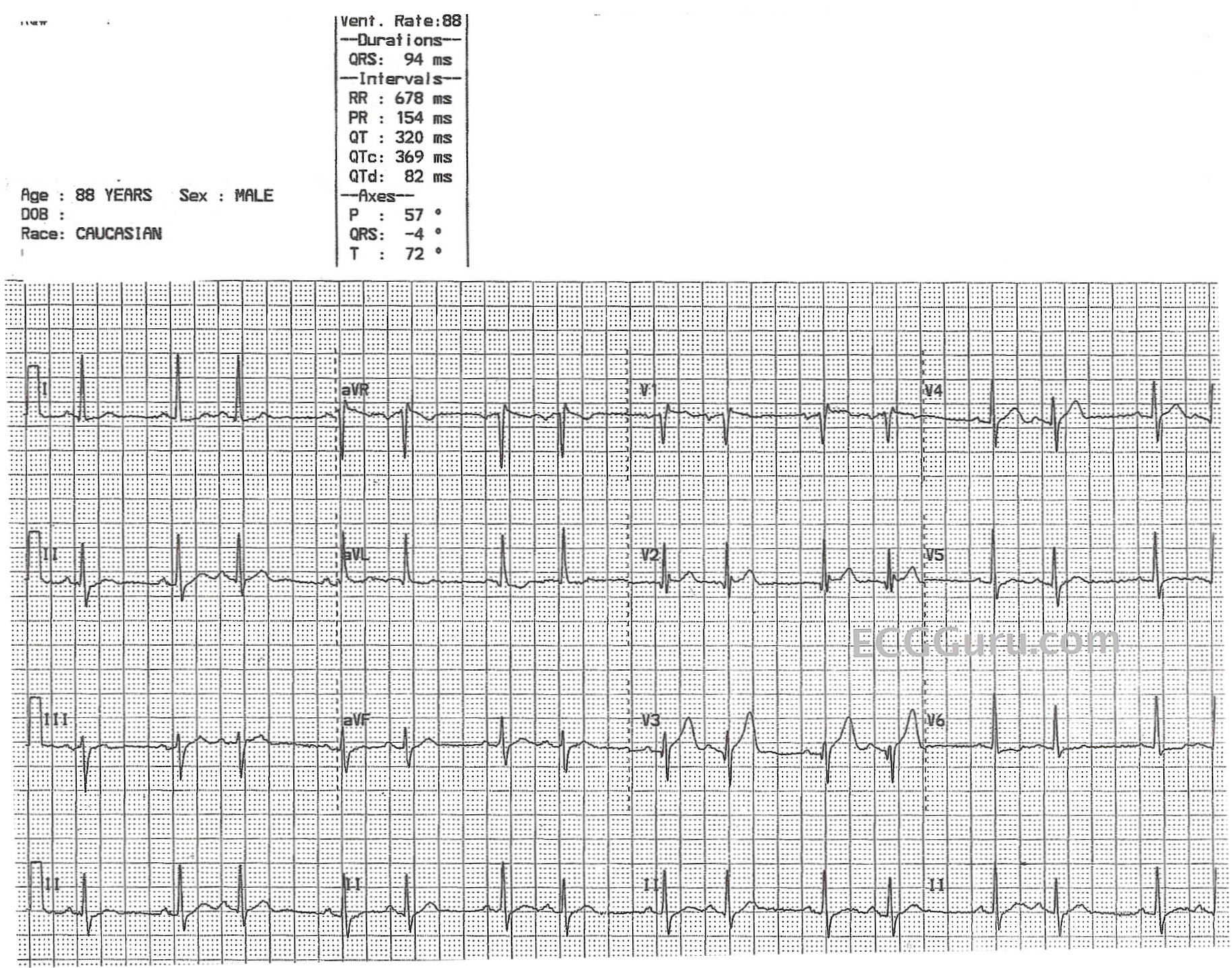
This ECG is from an 88-year-old man with congestive heart failure. No other clinical information is known. It shows an underlying sinus rhythm with atrial bigeminy - every other beat is a premature atrial contraction. There is very little, if any, difference in the morphology of the sinus P waves and the ectopic P waves, indicating that the ectopic focus is in the vicinity of the sinus node. There is no "compensatory" pause, because PACs penetrate the sinus node, resetting it. So, the underlying sinus rate here is about 72 beats per minute. There are several mechanisms for bigeminy to occur, but ectopic bigeminy is the most common.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Atrial Bigeminy — or Something Else? (ie, SA Wenckebach?)
Ken Grauer, MD www.kg-ekgpress.com [email protected]