
Submitted by Dawn on Fri, 12/20/2013 - 13:08
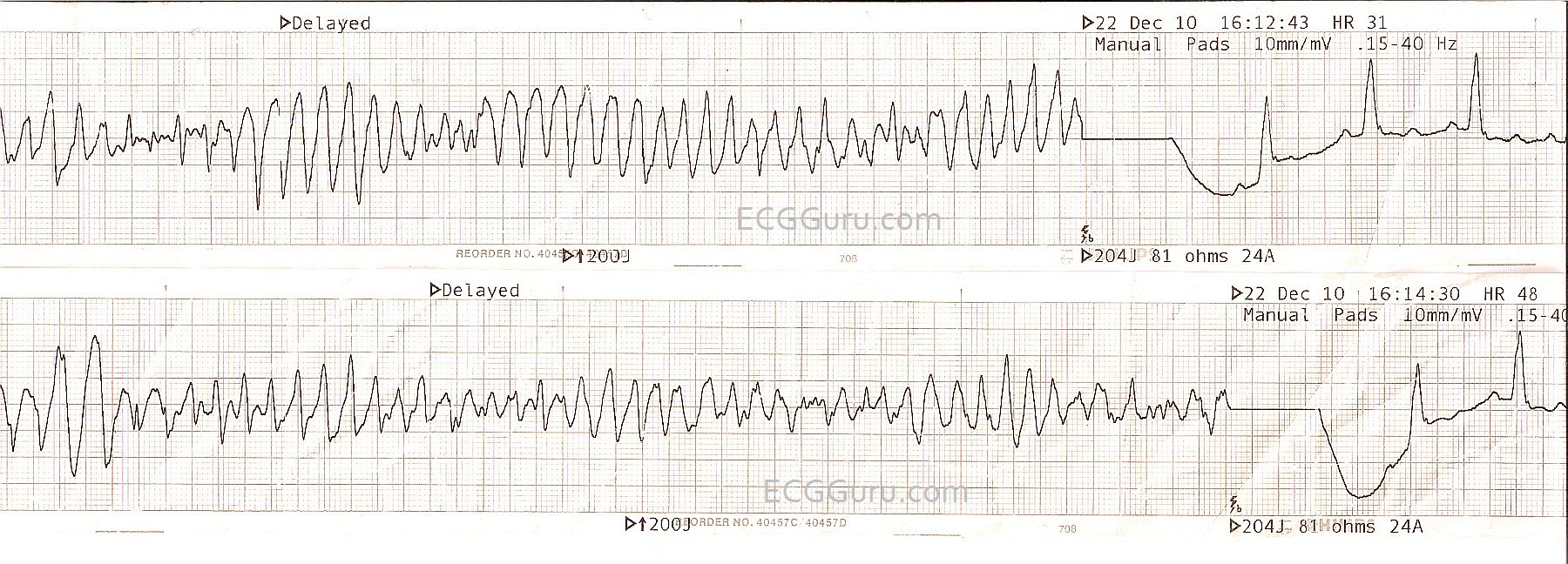
These two strips are from one patient who was electrically cardioverted twice in a few minutes. The original reason for the cardioversion was Torsades de Pointes, a type of polymorphic ventricular tachycardia associated with a long QT interval. For more information about TDP, go to this LINK. It is a bit difficult to comment on the patient's post-cardioversion rhythm, because so little of it is shown. It appears to be sinus, with a wide QRS. The QT interval appears slightly prolonged at .44 sec, but it is not known what the QT interval is corrected to a rate of 60/min. TDP is often seen with QT intervals greater than 600 ms (.6 seconds). Also THESE STRIPS ARE NOT SIMULTANEOUS, they were taken two minutes apart. In the first one, the P waves and T waves look so much alike, they could all be P waves. They do not "march out". It is necessary to get a long strip, preferably in multiple leads, and a 12-Lead ECG, to properly evaluate the rhythm post-cardioversion.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Torsades Converted - a "Picture Perfect" Example
The ECG posted by Dawn is a "picture-perfect" example of Torsades - in that there is true "twisting of the points" about the baseline. In each tracing - note slinky-like alternating of negative and positive deflections. Alas, we now require QT prolongation for qualify as "Torsades" vs PMVT (PolyMorphic Ventricular Tachycardia).
Ken Grauer, MD www.kg-ekgpress.com [email protected]