
Submitted by jer5150 on Sat, 07/05/2014 - 11:51
This is an ECG I performed a couple of years ago on an asymptomatic 83-year old man as an outpatient procedure.
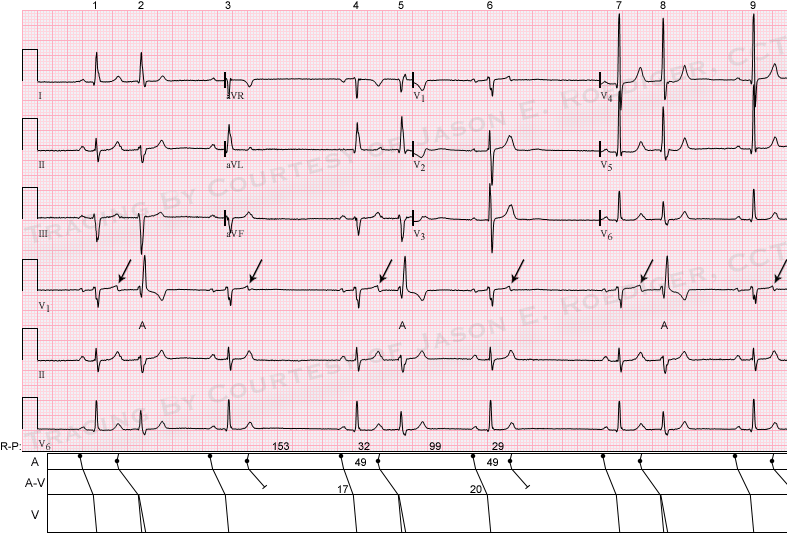
The computer interpreted this as: "Marked sinus bradycardia [with] Frequent Premature ventricular complexes". IS THE COMPUTER CORRECT? Is there more than one plausible interpretation? What is the differential diagnosis?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Atrial trigemeny
At first glance certainly appears to be a sinus brady with borderline first degree heart block - PR = 0.22. Narrow complex, regular ectopic activity in keeping with an atrial trigemeny. Also, voltage criteria indicative of LVH.
You cannot even spell it.
You cannot even spell it. Trigemeny indeed! Try bigemeny (so we understand each other), some non-conducted, some aberrant.
RBBB pattern and non-conducted PAC's
First of all, those premature complexes are aberrantly conducted premature atrial complexes (with RBBB configuration, because the right bundle branch isn't completely repolarized yet) and secondly there is at least 1 non-conducted premature atrial complex, partially hidden in the 3rd T wave and possibly one in the 6th as well.
SINUS BRADY, Ectopic trigeminy, Supernormal Conduction
Sinus Bradycardia atrial rate is constant at about 34bpm. Whether the ectopic beats are atrial or ventricular I cannot tell from this ekg(correction relatively narrow qrs in lead 1 suggest that the ectopic beat is of atrial or avnodal origin). Whichever it is there is no compensatory pause after each ectopic beat. As a matter of fact the Sinus p waves are coming in faster than expected after the ectopic beat. A premature atrial complex that has supposed captured the atrium is not reseting the cycle. Supernormal conduction?
I would be interested in the correct interpretation, and would like to send you one i have that's similar to this; Atrial rate at 75bpm with clear atrial ectopic beats that do no affect the sinus cycle at all.
Contact info
"Chireu",
If you'd like to send me your ECG or rhythm tracing, I'll take a look at it an get back with you. My email is [email protected]. You'll have to click directly on my email to bypass the SPAM detector.
Jason
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
ABERRANT BEAT
The ECG shows Marked sinus bradycaria with aberrant premature beats. The premature beat can be seen on V1 as triphasic having a RBBB morphology. This atrial prematurebeat occured while the right bundle branch is in refractory period giving it a RBBB morphology.
PAC's with aberrancy in a pattern of trigeminy
If you put your calipers to the sinus p waves, and forget about the premature beats for a moment, all the beats map out. I am thinking that the PAC did not reset the SA node, possibly because the SA node had time to repolarize. That is why there is a shorter pause after the PAC than after the sinus beat.
Still not satisfied
I agree with the sinus bradicardia, and that the premature beats are atrial in origin and aberrant, but the lack of resetting of the sinus pacemaker disturbes me. I think that an explanation is that there is a PAC conducted and the next nonconducted and so on in able to explain what we see in this strip.
atrial bigeminy
Sinus rhythm (rate unknown) with atrial bigeminy. The atrial premature beats are alternately conducted with a RBBB+left anterior fascicular block pattern and non-conducted. Those conducted with a RBBB/LAFB pattern also have a long PR interval, suggesting the possible presence of dual AV nodal pathways with block in the fast pathway on these beats. It is impossible to say what the underlying sinus rate is because there are not two consecutive sinus beats. Unusual ECG!
Dave R
Dave R....Couldn't the long
Dave R....Couldn't the long pr interval and abbarent conduction of the first pac in the cycle be related to the subsequent non conducted pac? The first one had difficulty conducting and the next one couldn't? But if that is so....why? The R to R interval preceding the abberantley donducted beat is shorter than the R to R interval preceding the blocked PAC. That would rule out refracory issues unless some concealed conduction is also lurking.Puzzeling
Dan
Dan
Interpretation?
Jason, can you give us the interpretation for this ECG? Thanks!